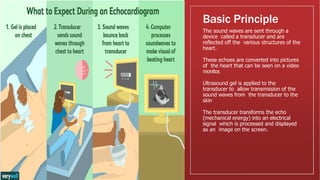
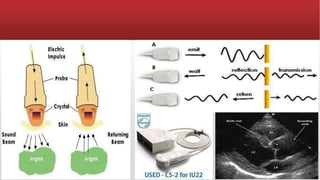
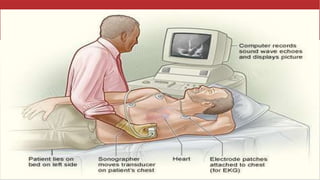
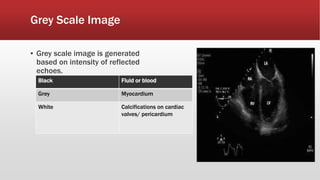
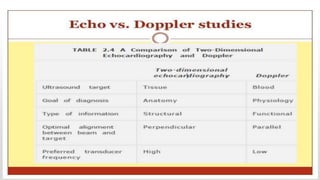
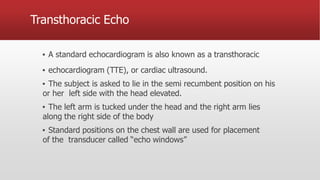
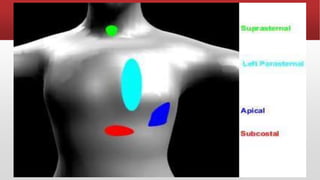
Echocardiography is a non-invasive ultrasound test that creates images of the heart using sound waves, allowing assessment of cardiac structure and function without radiation risks. It includes various modalities such as 2D, M-mode, and Doppler echocardiography, which cater to different diagnostic needs in clinical cardiology. The procedure can be performed using transthoracic, transesophageal, and other approaches, providing significant information about both structural and functional aspects of the heart.