Downloaded 123 times
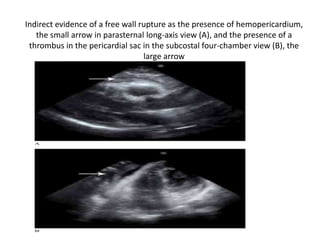
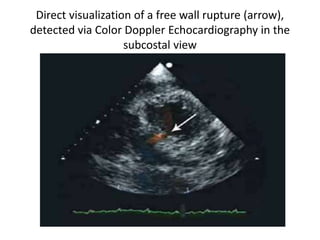
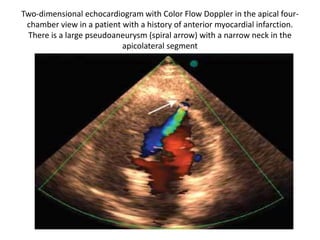
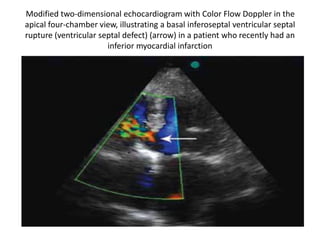
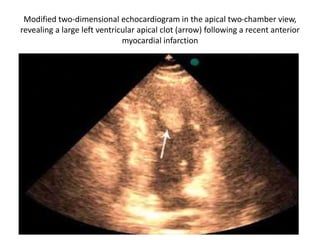

Echocardiography plays an important role in diagnosing ischemic heart disease through evaluating wall motion abnormalities, localizing infarcts, assessing infarct size, and detecting complications. It can detect abnormalities such as ventricular rupture, pseudoaneurysms, ventricular septal defects, and clots. Stress echocardiography enhances interpretation of stress tests and evaluates functional importance of coronary artery disease. Echocardiography is accurate for evaluating patients with known or suspected coronary artery disease.























































































