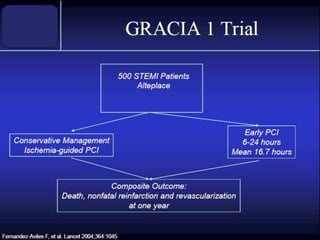
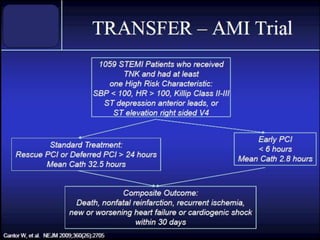
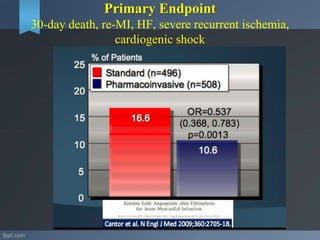
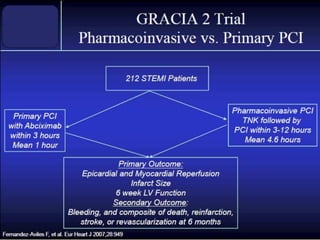
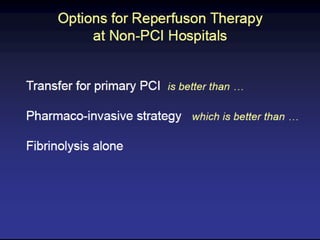
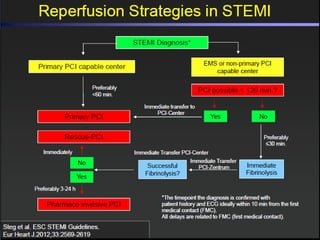
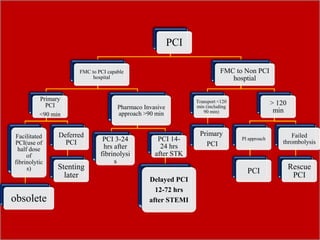
1. The document discusses the pharmaco-invasive approach for patients presenting with ST elevation myocardial infarction (STEMI) in India. This approach involves initially administering early fibrinolytic therapy followed by angiography and percutaneous coronary intervention (PCI) within 3-24 hours, regardless of the success of fibrinolysis.
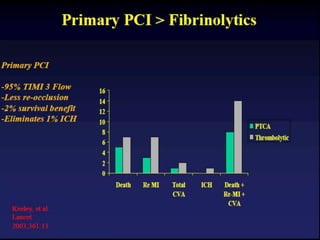
2. It highlights challenges with the current STEMI system of care in India such as lack of awareness, limited transfer facilities to PCI-capable hospitals, and delays in initiating reperfusion therapy. The pharmaco-invasive approach aims to shorten time to reperfusion of the infarct-related artery.
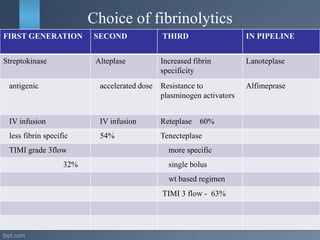
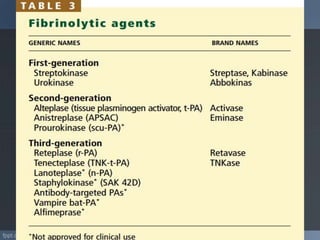
3. Guidelines for the pharmaco-invasive approach in the Indian setting are provided, including recommendations on agent choice


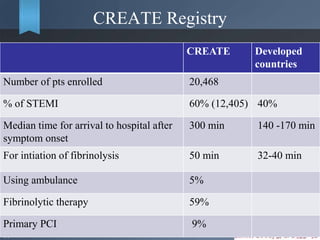
![Indications
• It is appropriate for patients with STEMI who are eligible for
treatment with fibrinolytics drugs and in whom
Transfer time ≥30 min, or
DTB(door to balloon) time≥90 min,
[FMC to balloon time > 120 min].
• PCI related delay : (door to balloon) – (door to needle) > 60
minutes.
Shortening the time to reperfusion of the Infarct related artery.
Optimal reperfusion strategy for patients with STEMI.](https://image.slidesharecdn.com/pharmacoinvasiveapproachforstemi-151112095429-lva1-app6891/85/Pharmacoinvasive-approach-for-stemi-44-320.jpg)




















































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)

















