



![PredicEve
Scores
TASH
(Trauma
Associated
Severe
Hemorrhage)
7
independent
variables.
Punctua$on:
0-‐28.
-‐
Each
punctua$on
represents
a
%
of
massive
transfusion
(MT).
-‐Equa$on:
p
=
1
/
[1
+
exp(5.4
–
0.3
x
TASH)]
TASH>
16
→
MT
>
50%
TASH>
27
→
MT
100%
Maegele
M.
Transfusion
Medicine
and
Hemotherapy
2012;
39:85-‐97.
Maegele
M.
Vox
Sanguinis
2011;
100:231-‐238.](https://image.slidesharecdn.com/massivetransfusionprotocols-170118161033/85/Massive-transfusion-protocols-13-320.jpg)


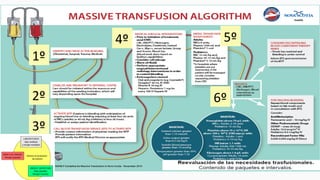
![Administrar: A. Tranexámico Bolus 1g +bomba infusión
continua (1g/40ml SF) a pasar en 8h (5ml/h)
Mantener: Ta>35oC;Ph>7,2;Ca>1mmol/l;Hb>8 gr/l
Analizar: TP;TTPA; Reptilase;PLQ; Fibrinógeno+EXTEM;INTEM
Normal
Desmopresina 0,3ug/Kg
1 pool Plaquetas
STOP
SANGRADO
Repetir pruebas después de cada tratamiento
¿Antivitaminicos K?
Rotem: ML>15% en 1h y corregido en APTEM
Rotem: MCF [(Extem<45 + Fibtem ≥ 8mm) ó Ex<33mm]
N° PLQ <50 x 109/L
Rotem: MCF (Extem<45 + Fibtem< 8)
Lab: Fibrinógeno<1,5 g/L
Rotem: CT Extem>80 y/o CTIntem>240
Lab: TP/TTPa>1,5Anormal
Coagulopatía
INR > 1,5 15UI/Kg. à CCP
INR >3 ó ? à 30 UI/Kg.
¿Sangrado
quirúrgico?
¿Disfunción Plaquetas?
Revisión
quirúrgica
Diagnóstico
diferencial
P. laboratorio
FIBTEM / HEPTEM / APTEM
Fibrinógeno
Plasma
15-30 mL/Kg
CCP
15-30 UI/Kg
FVII
90 µg/Kg
Plaquetas
1 pool
TMX 1 g
Rotem: CT Heptem < CT Intem
Lab: TTPa>1,5 + Trombina>60 + Reptilase Normal.
Protamina
1:1](https://image.slidesharecdn.com/massivetransfusionprotocols-170118161033/85/Massive-transfusion-protocols-29-320.jpg)






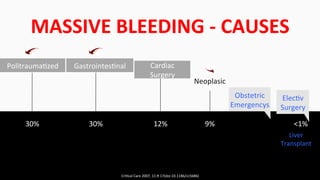
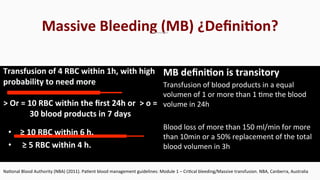
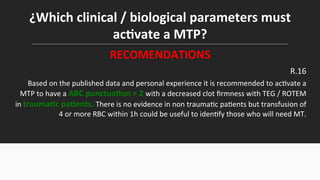
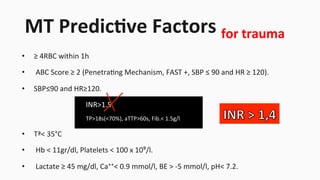
This document discusses protocols for massive transfusion and bleeding. It defines massive bleeding and massive transfusion, and explores ways to predict which patients may experience massive bleeding through the use of predictive scores and clinical/biological parameters. Predictive scores discussed include TASH and ABC scores. The document recommends activating a massive transfusion protocol for trauma patients with an ABC score >2 and decreased clot firmness on viscoelastic tests, or for non-trauma patients transfused with ≥4 RBC within 1 hour. Clinical parameters that could activate a protocol include low SBP/high HR, coagulopathy signs, low temperature, anemia, and lactic acidosis.





































































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)




