This document contains 17 questions about ECG interpretations with corresponding answers. Each question provides an ECG reading and clinical scenario, and the answers analyze the ECG findings and provide a diagnosis. Some of the conditions addressed include atrial fibrillation, atrial flutter, ventricular tachycardia, STEMI, non-STEMI, Brugada syndrome, WPW syndrome, hyperkalemia, pulmonary embolism, pericarditis, hypothermia, and more. The document serves as a teaching aid with examples of ECG interpretations for various cardiac conditions and presentations.










































![Answer
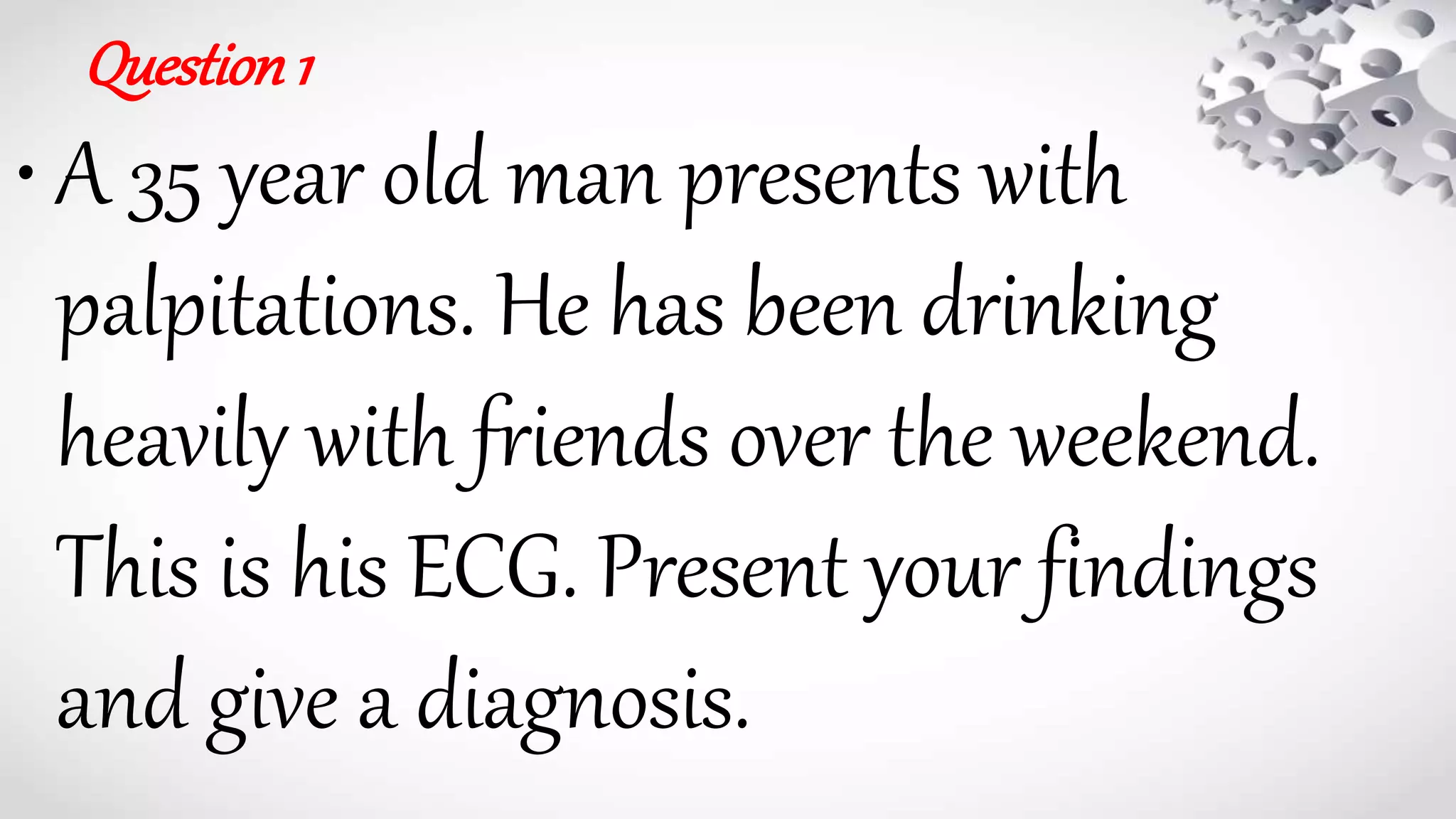
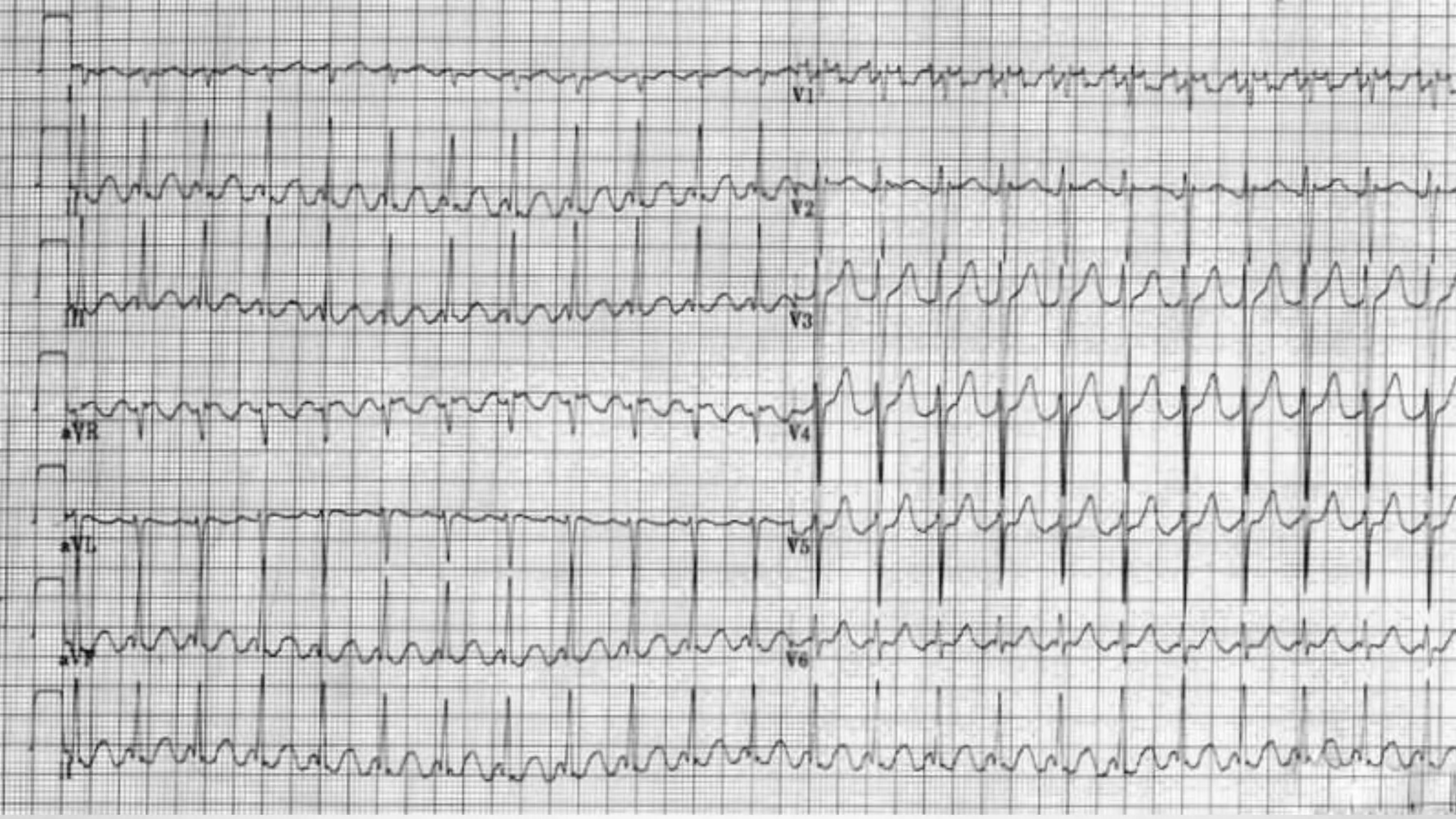
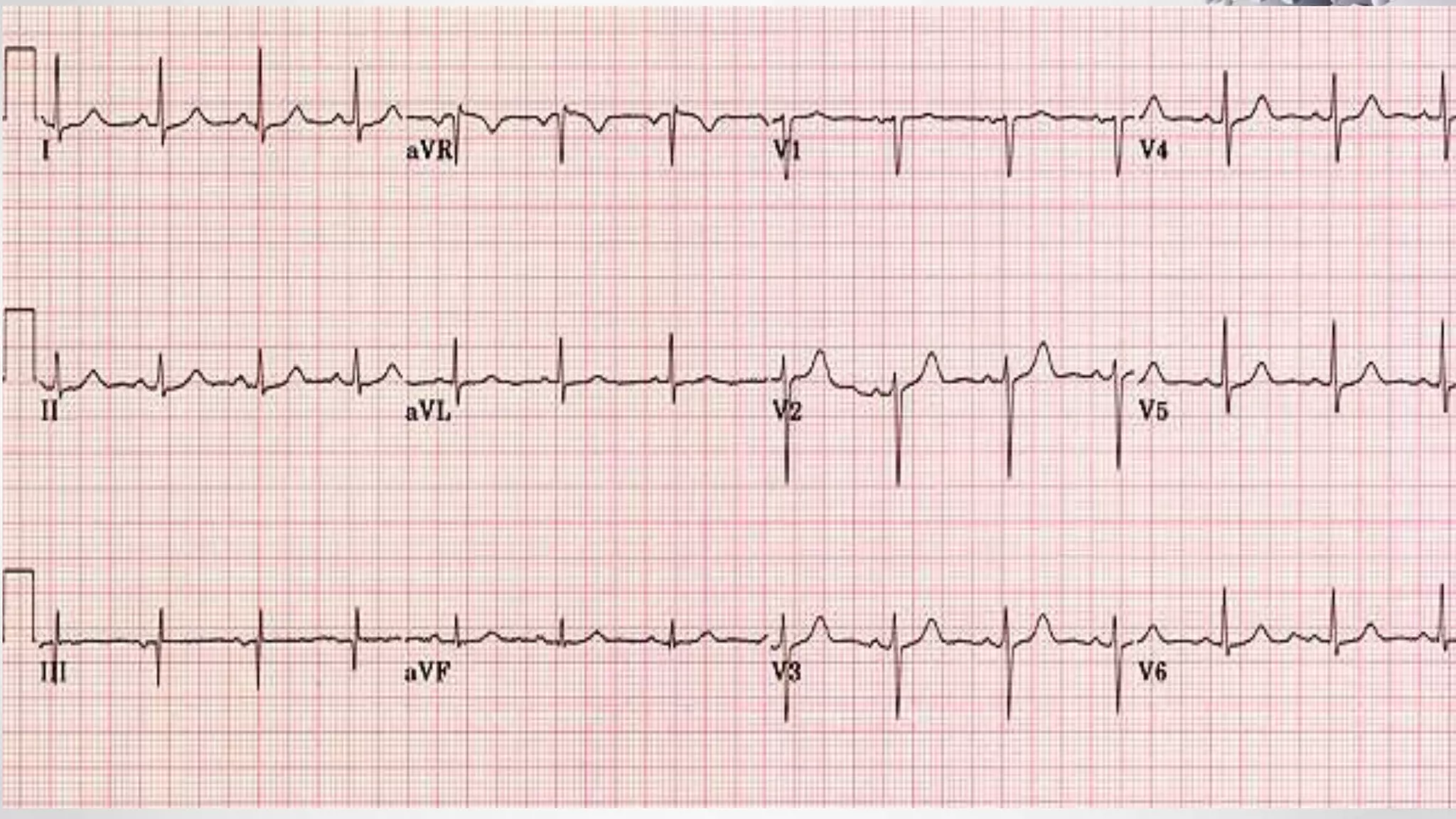
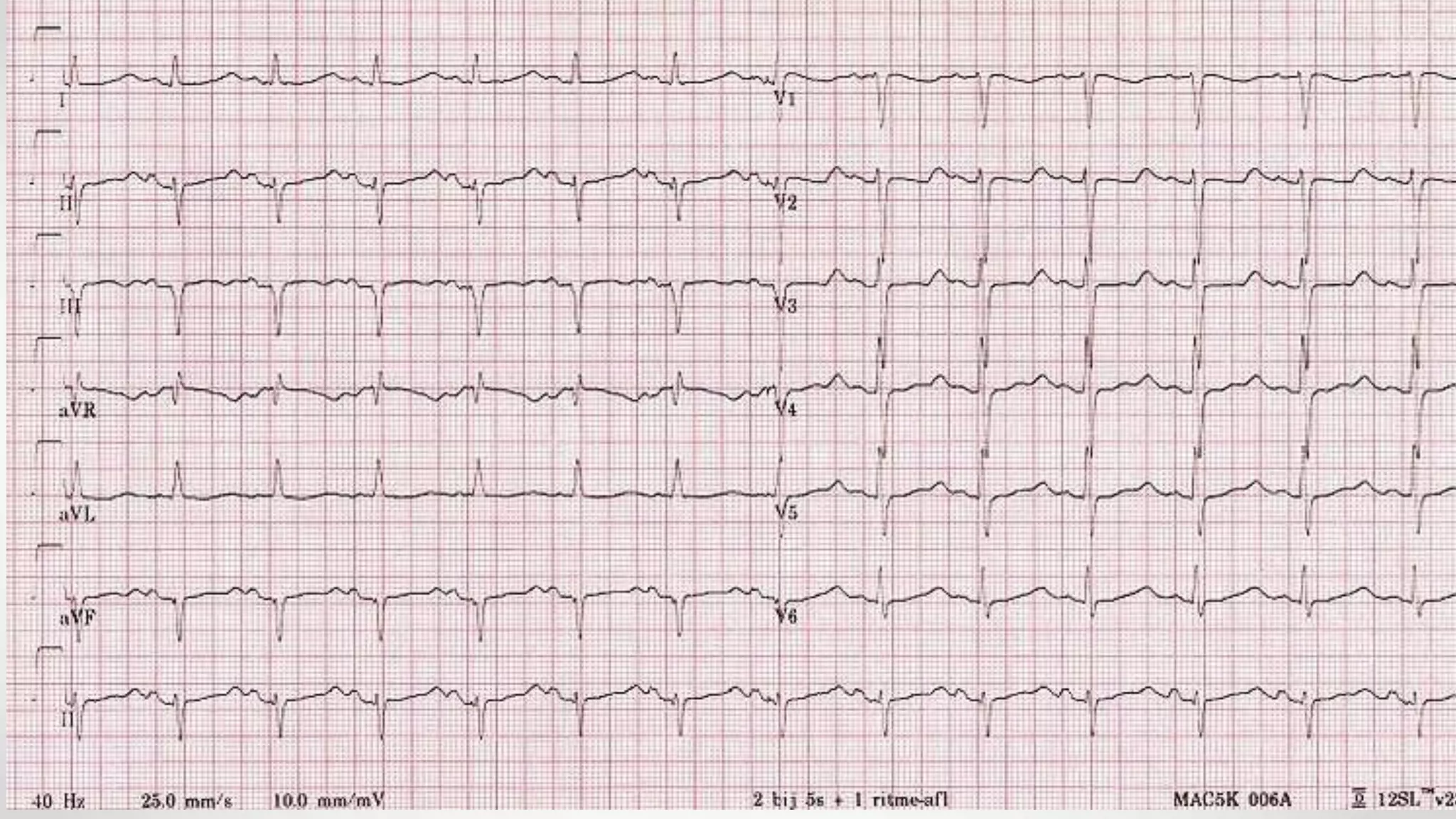
• Rate 85 .... Rhythm Regular ........ PR/P wave Unable to assess ............... QRS Wide
• ST/T wave Wide ............... QTc/other Prolonged
• Diagnosis:
1. The diagnosis is tricyclic antidepressant overdose. This causes widening of the QRS complex and
lengthening of the QT interval due to blockade of sodium channels. 2. [/toggle_item]
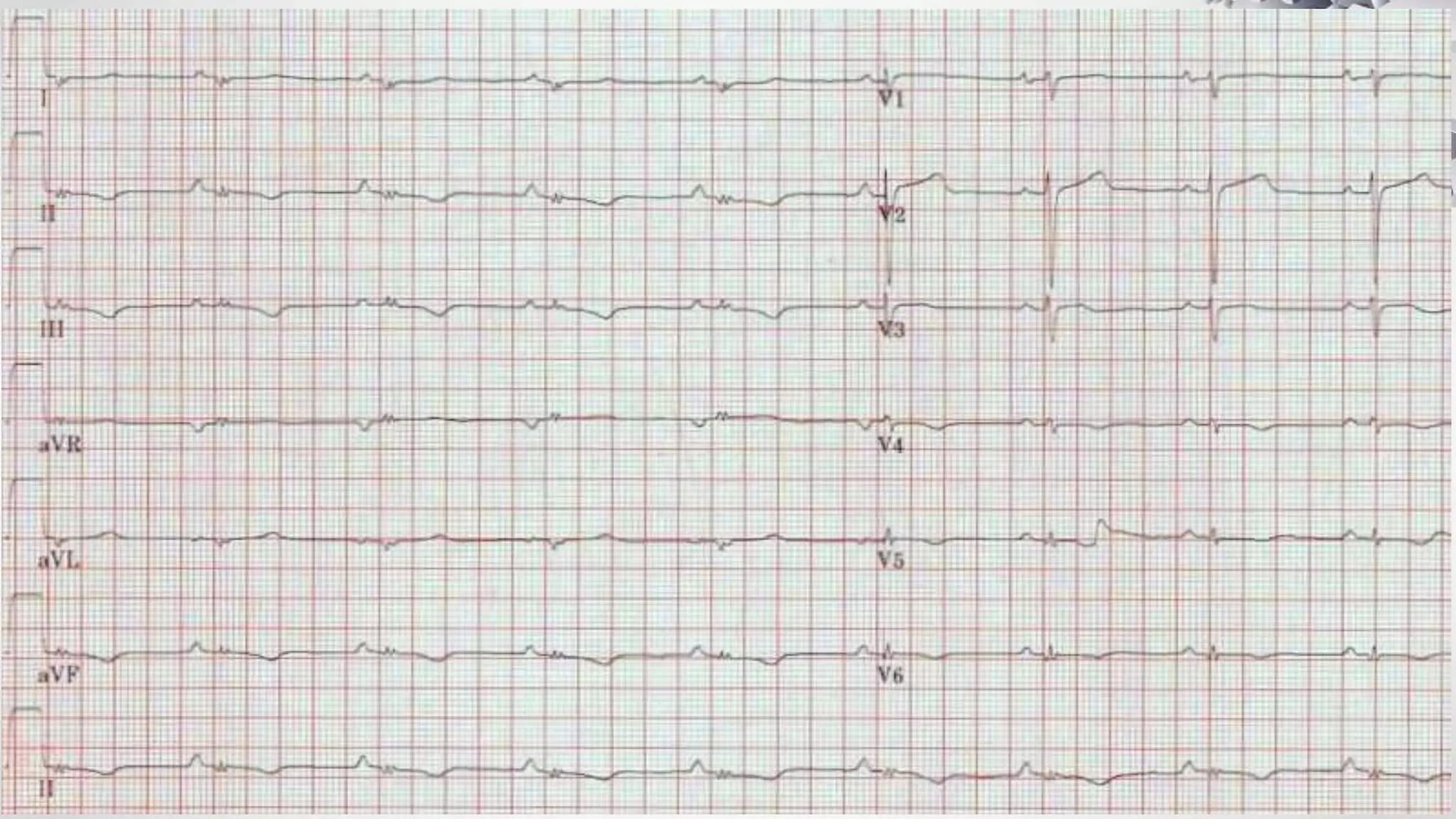
3. [toggle_item title=”What would you do?” active=”false”].......4. A,B,C,D,E (ventilation may be required)
5. Bloods including paracetamol level; ABG (likely metabolic acidosis) .6. Activated charcoal if within 8hrs of
ingestion
7. Sodium bicarbonate (50ml of 8.4%).. 8. Give if any arrhythmia or QRS>110
Further options:
If ventricular tachycardia: lignocaine (avoid beta blockers, amiodarone and calcium blockers)
If seizures: benzodiazepines](https://image.slidesharecdn.com/ecgexample-180401071123/75/Ecg-example-64-2048.jpg)