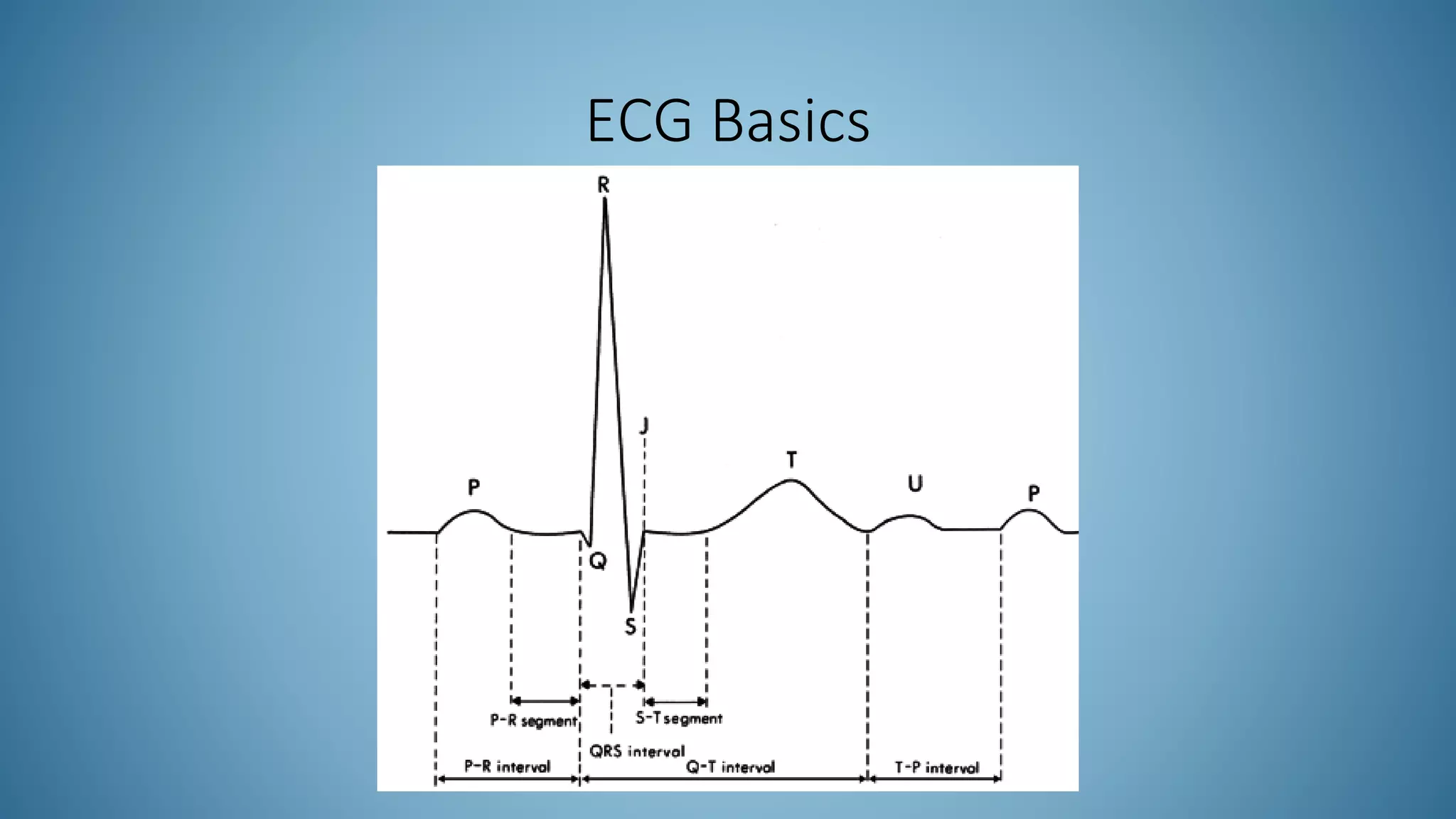
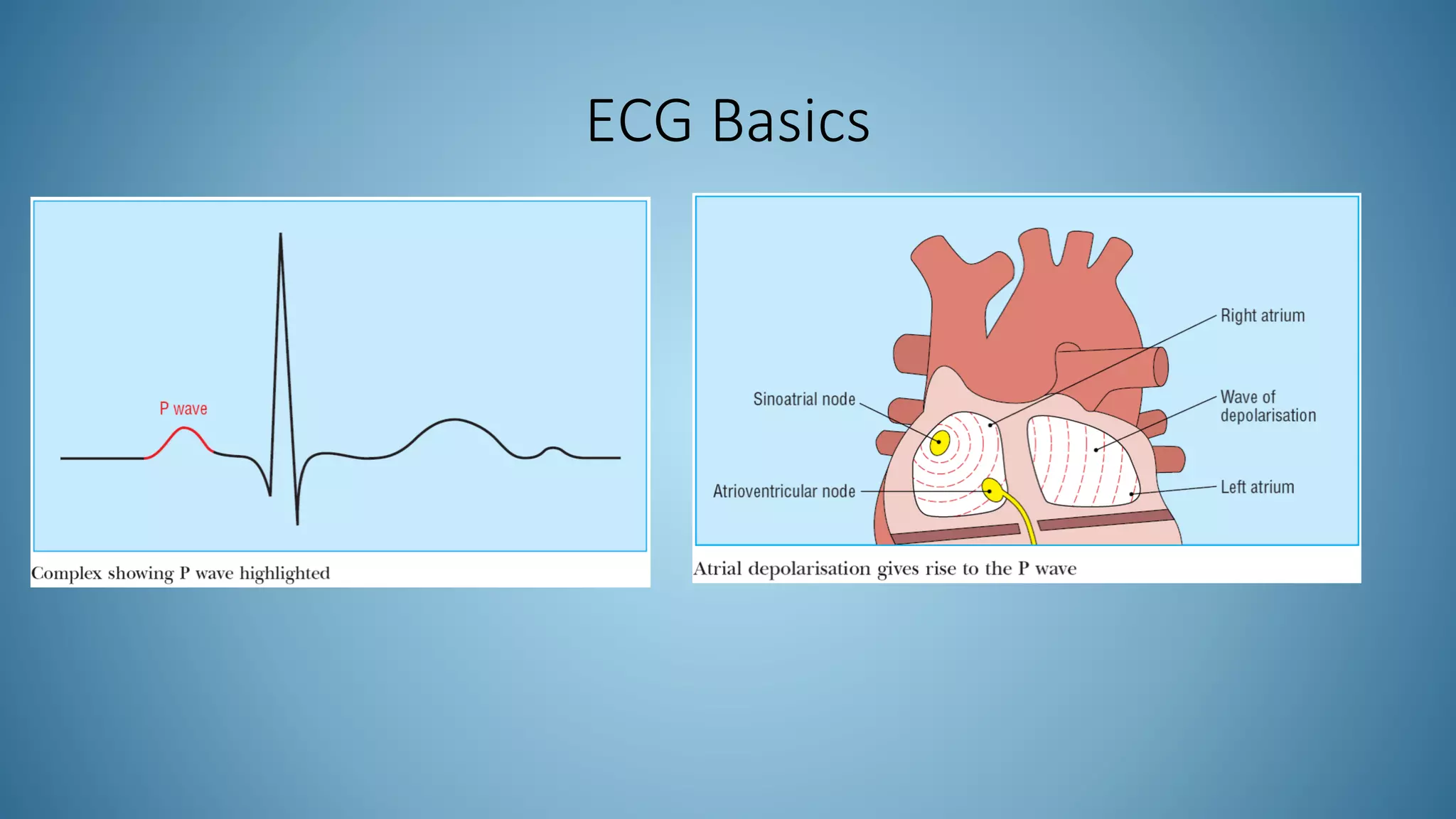
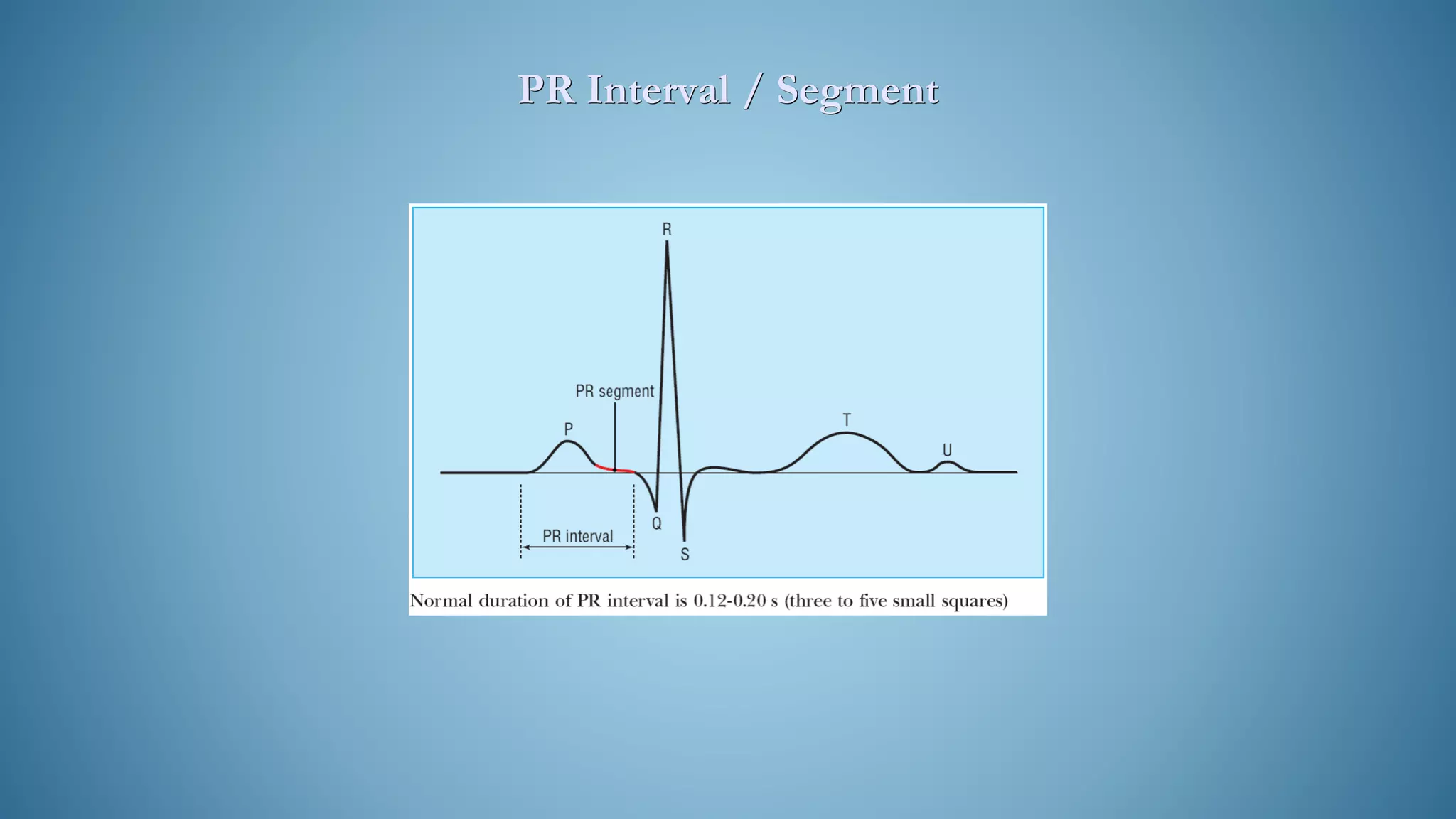
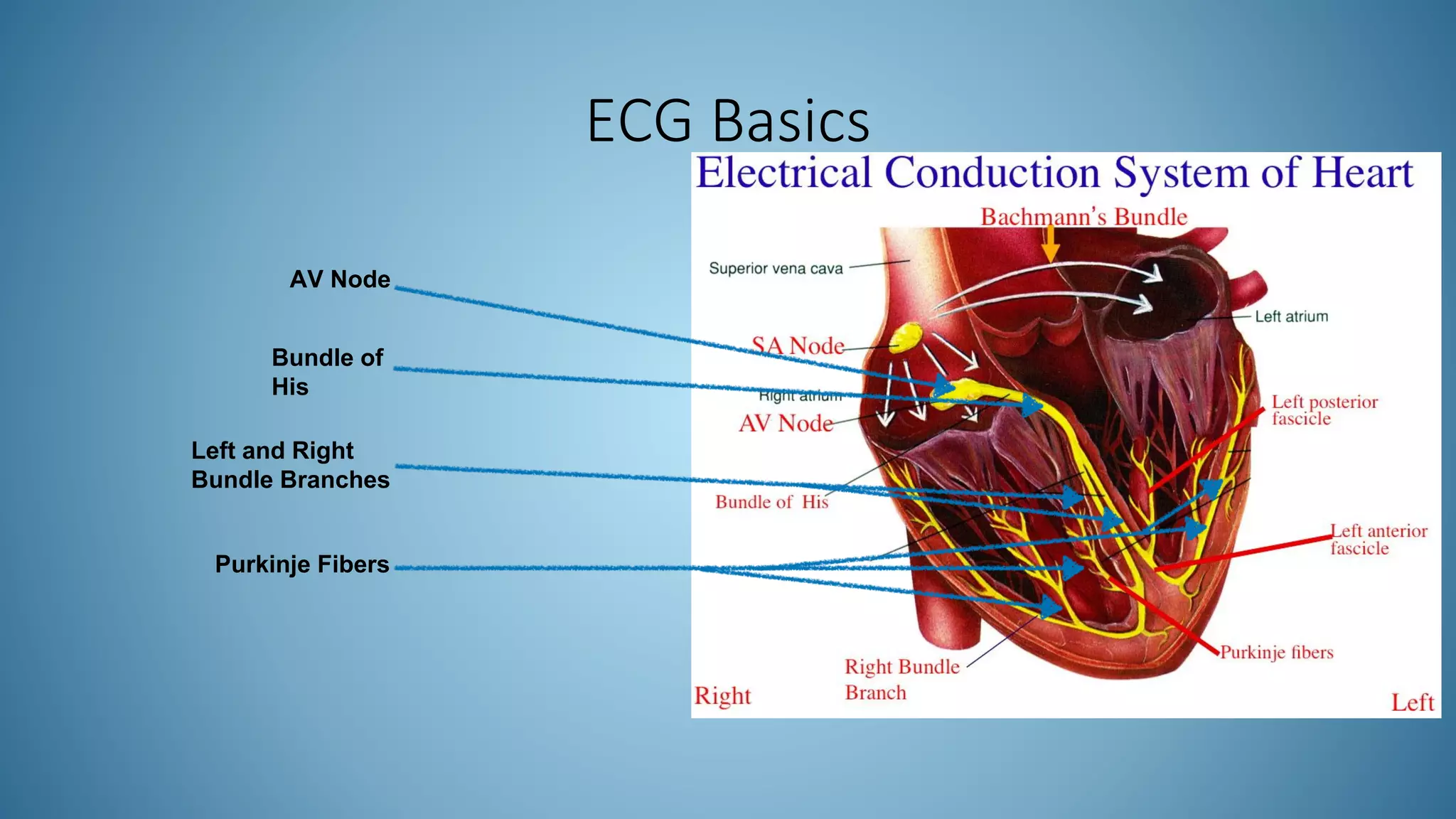
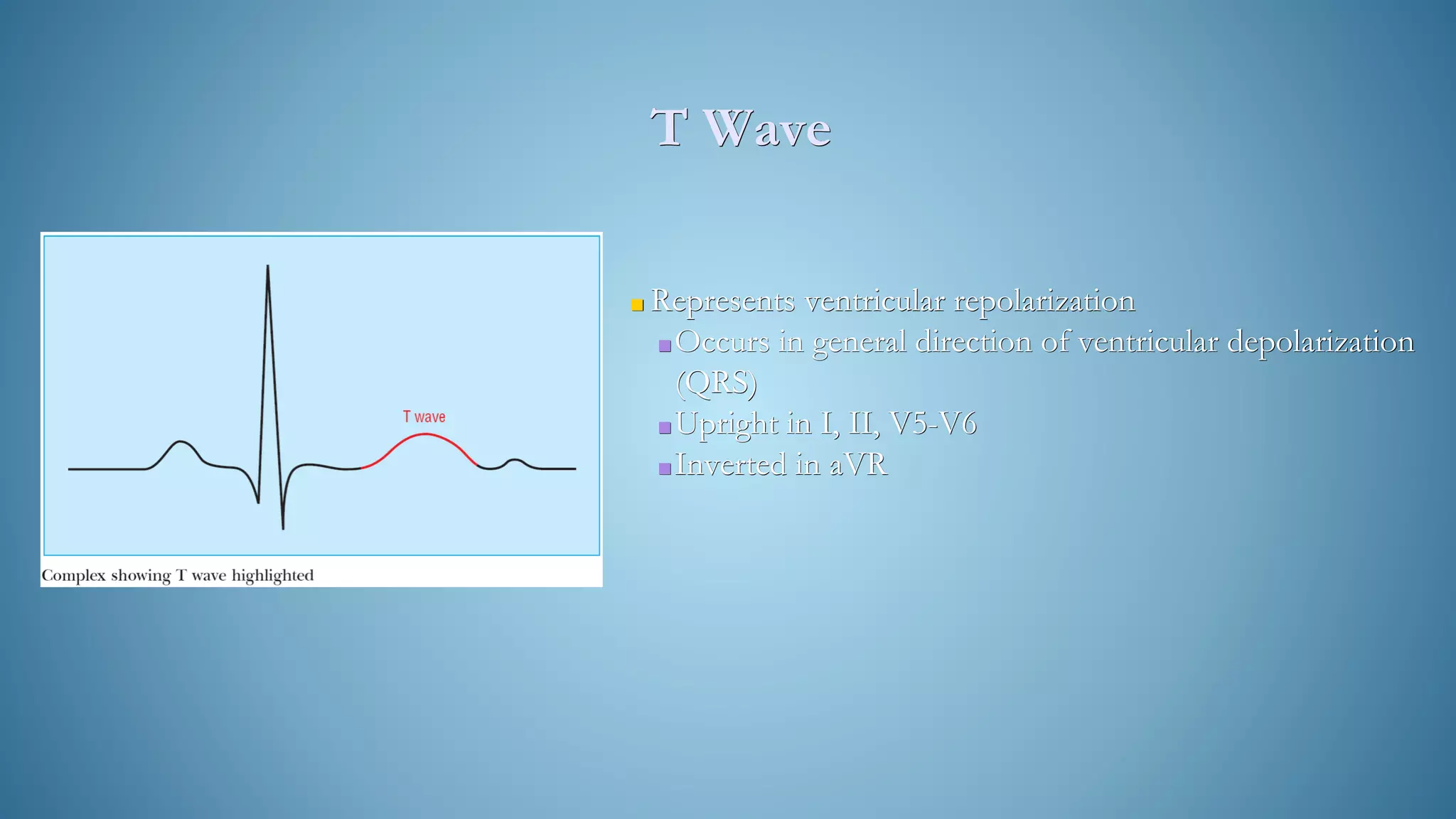
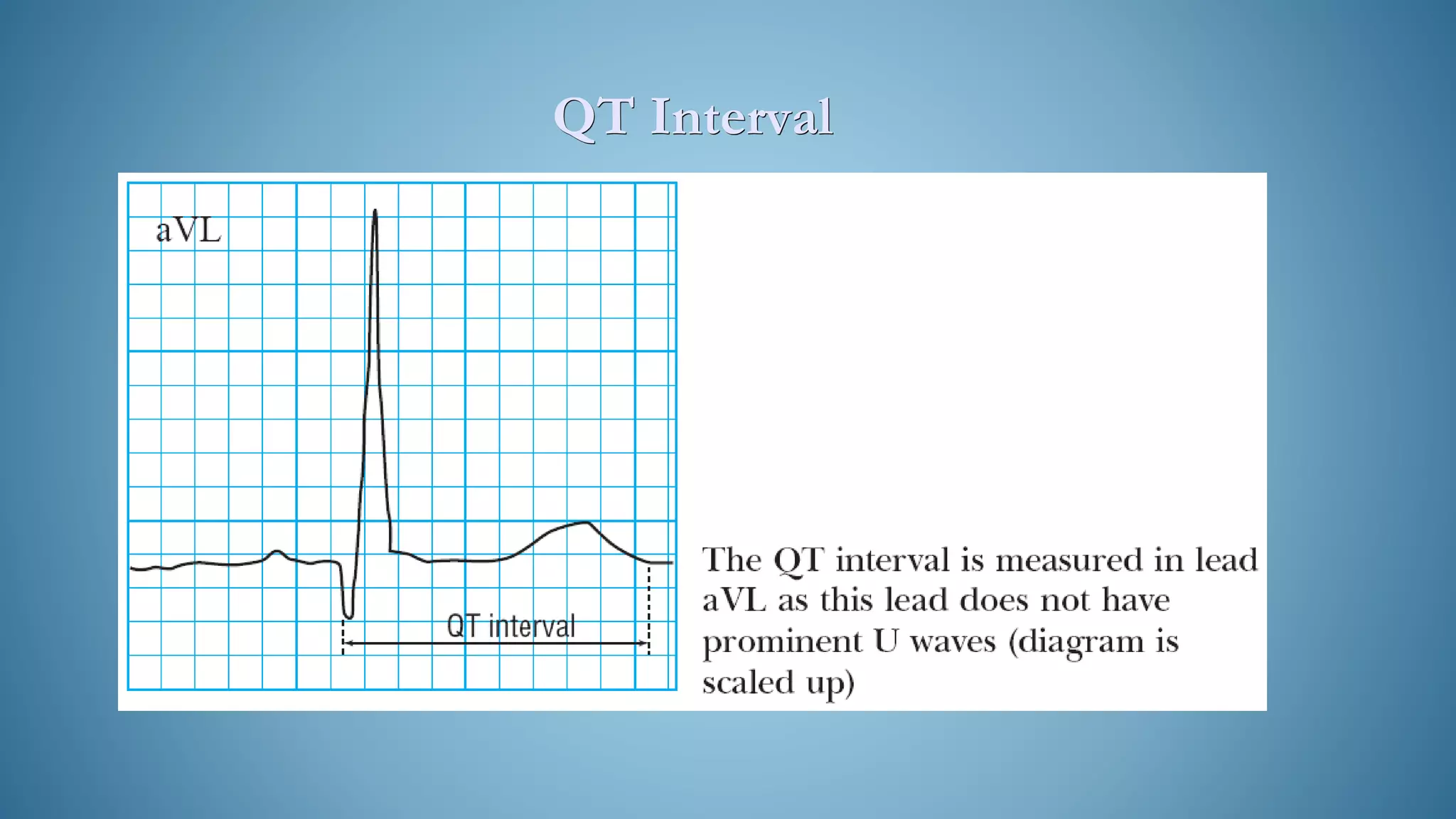
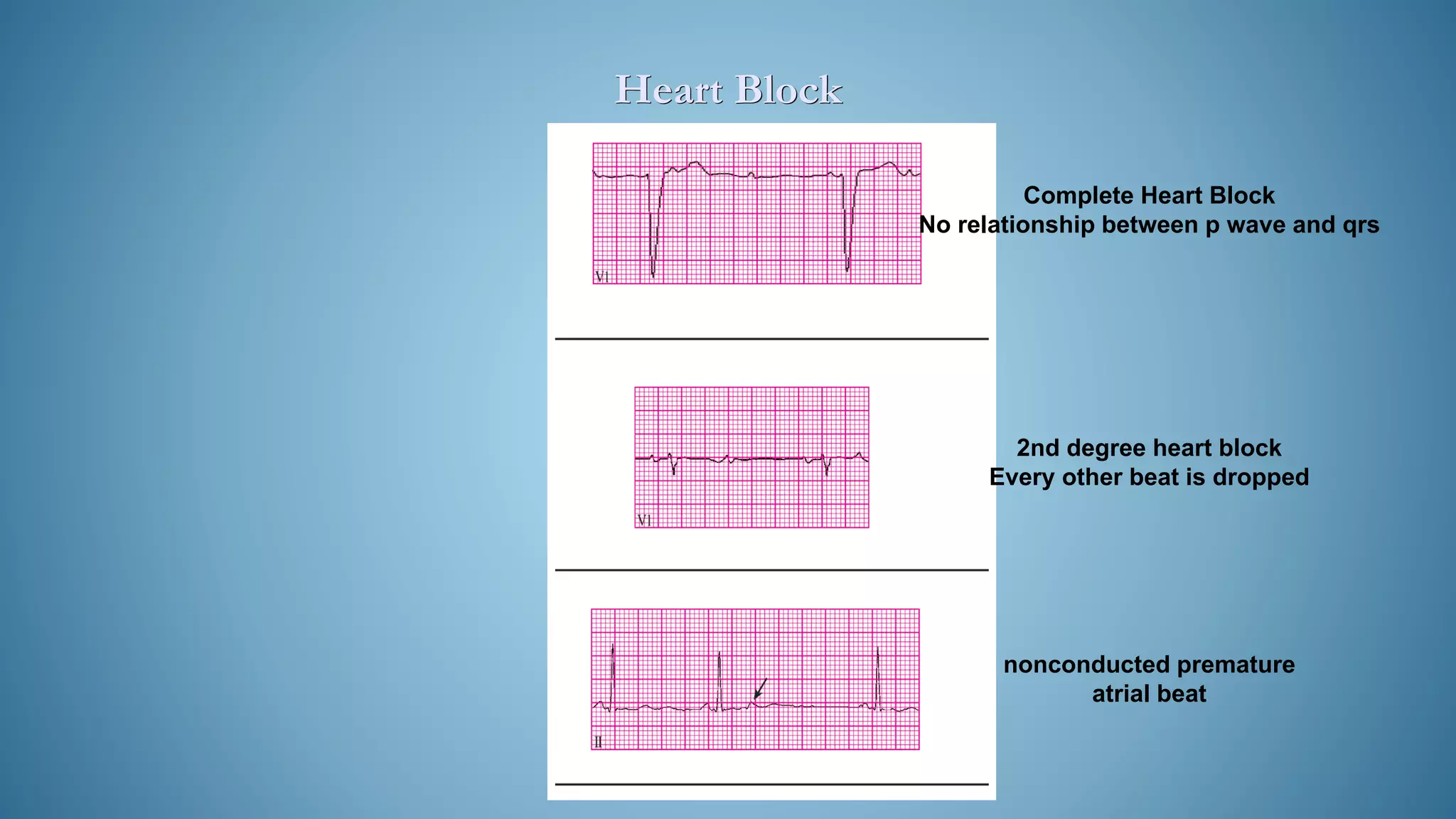
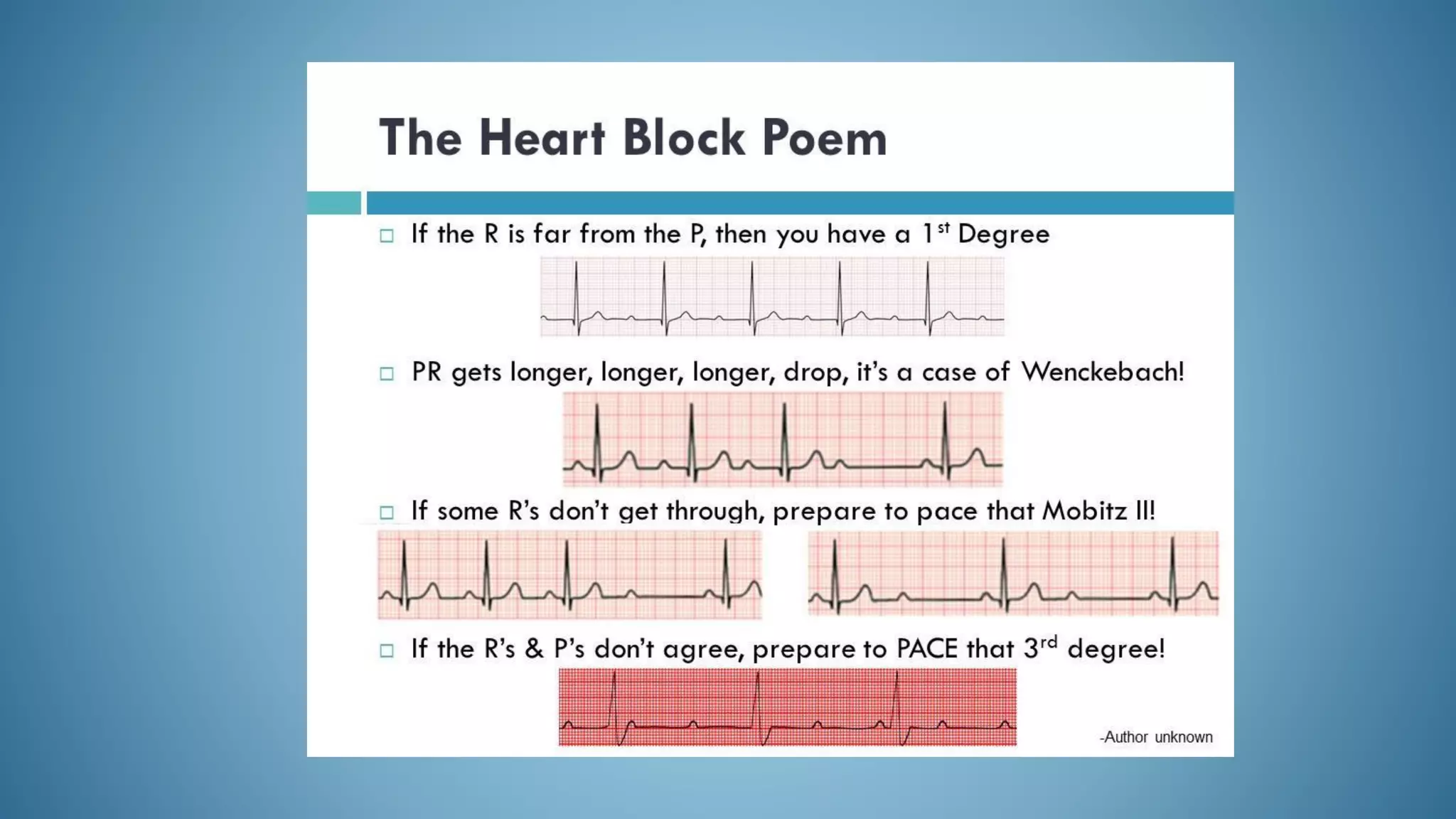
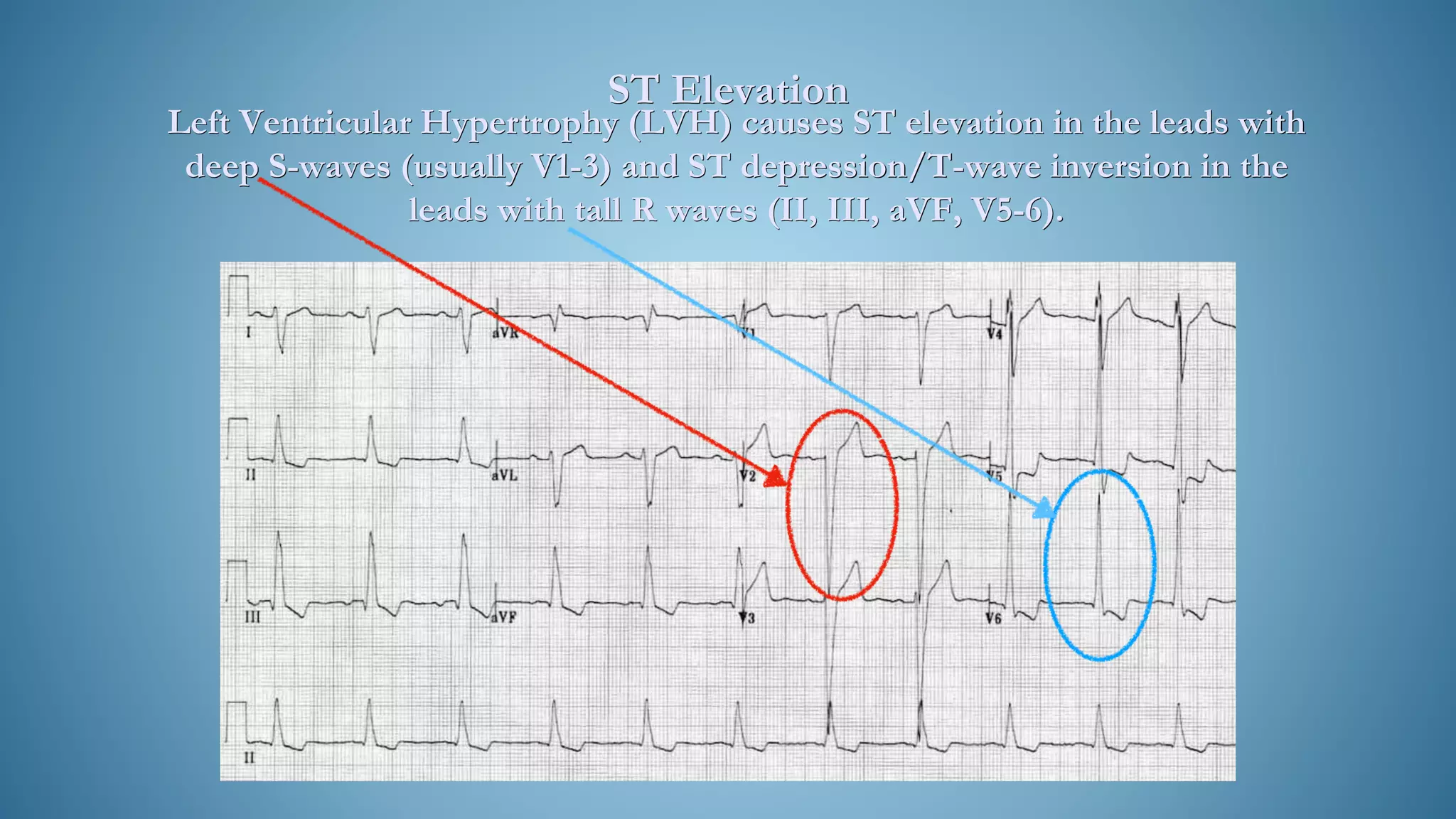
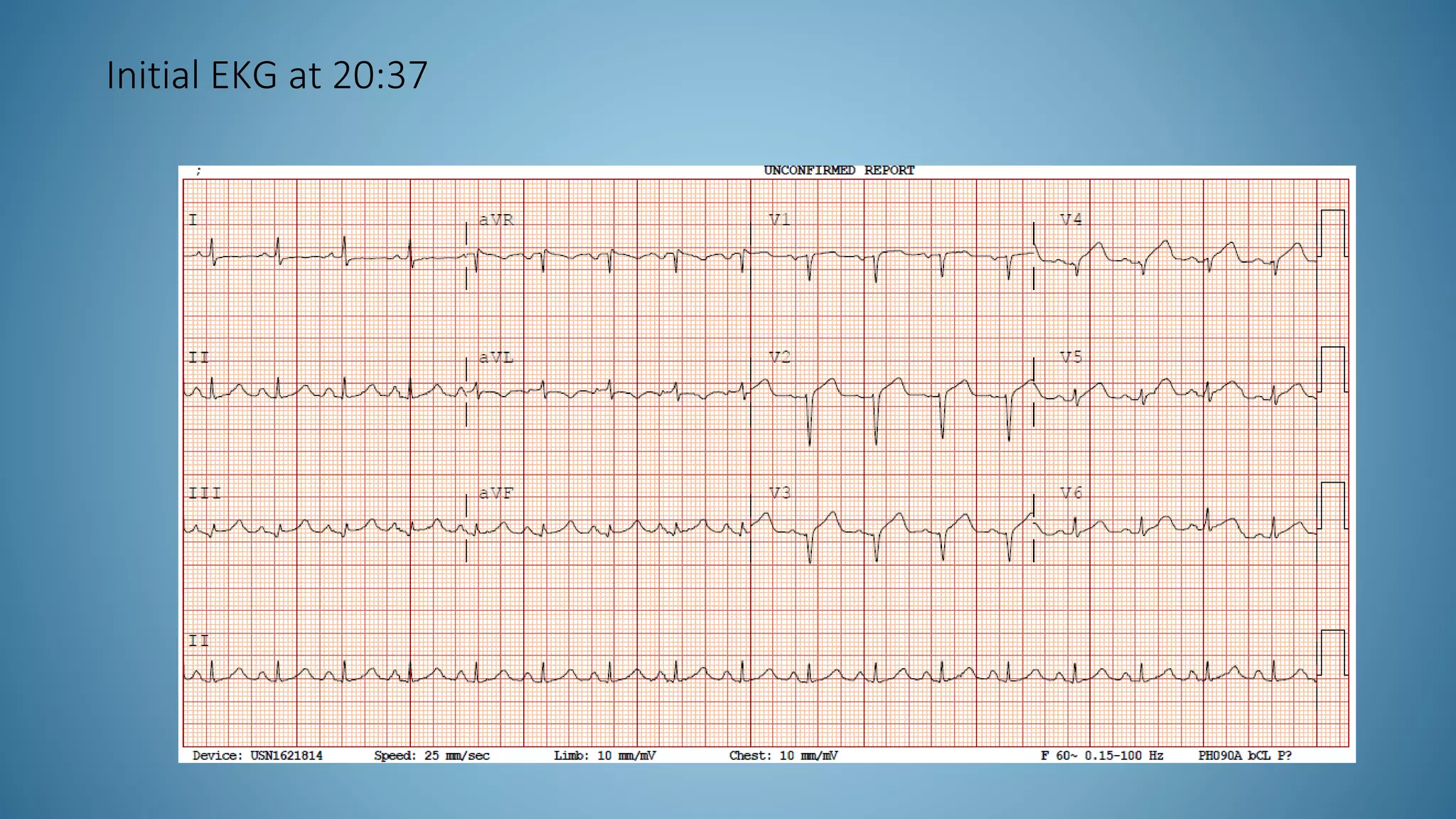
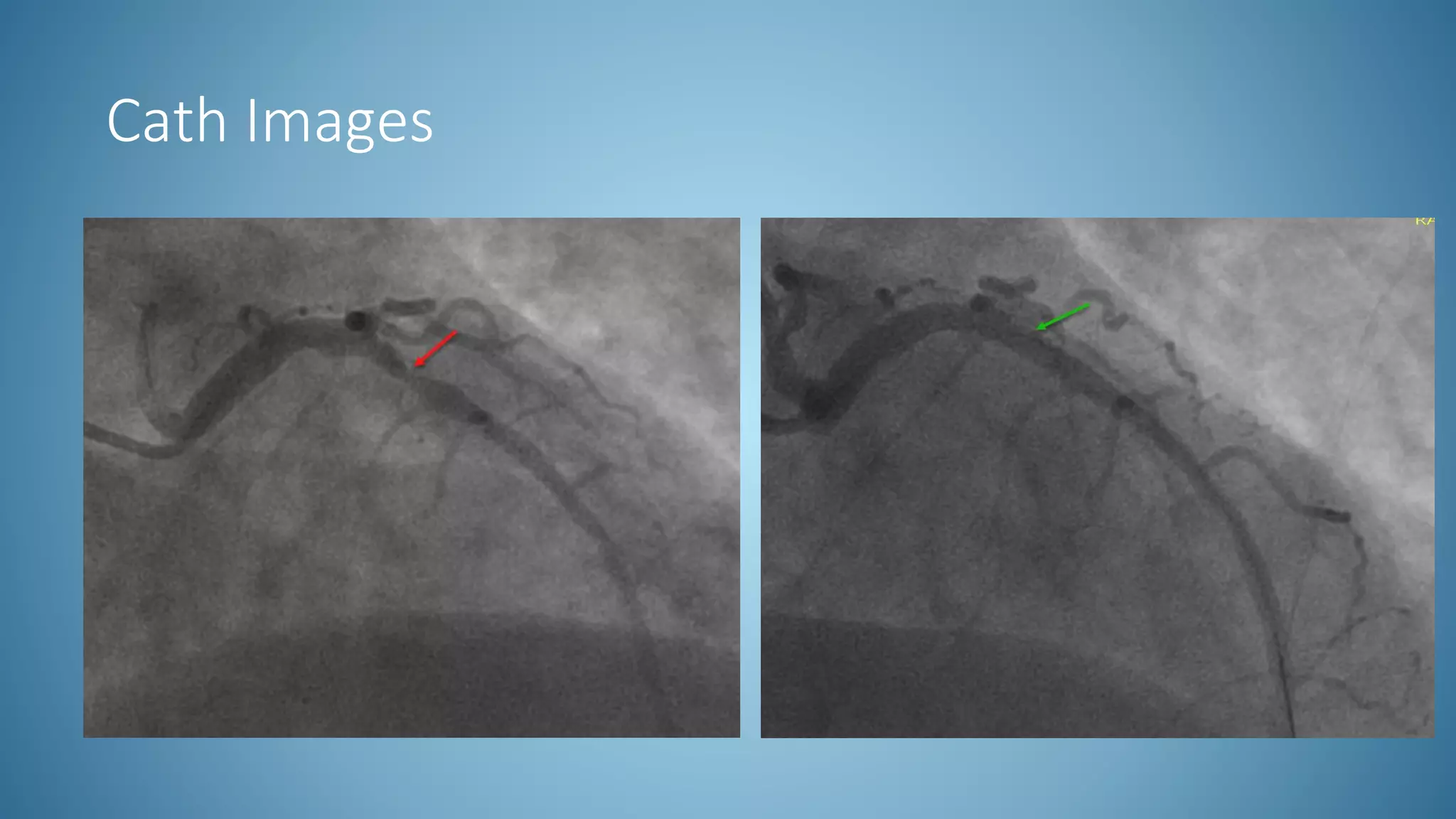
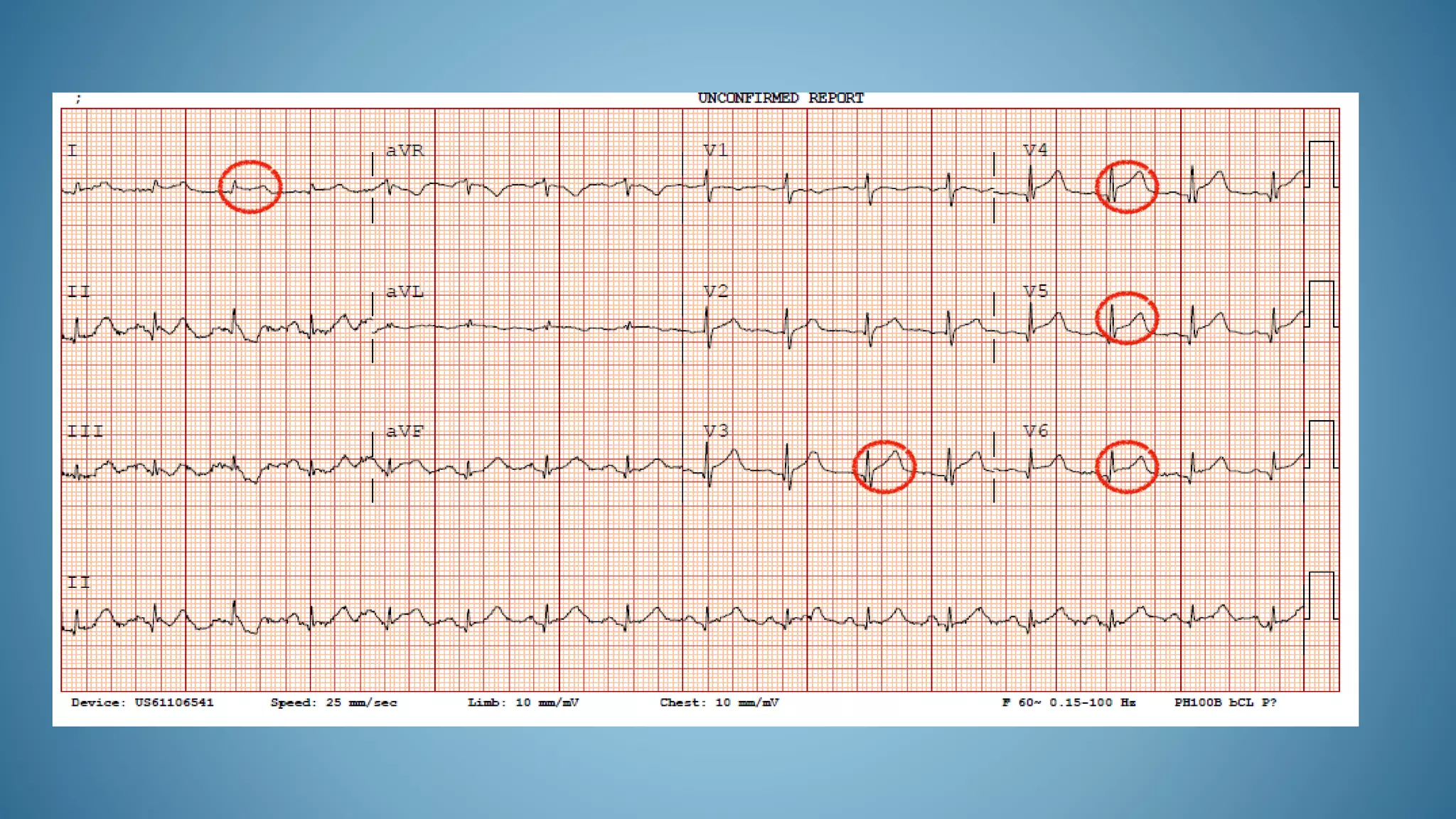
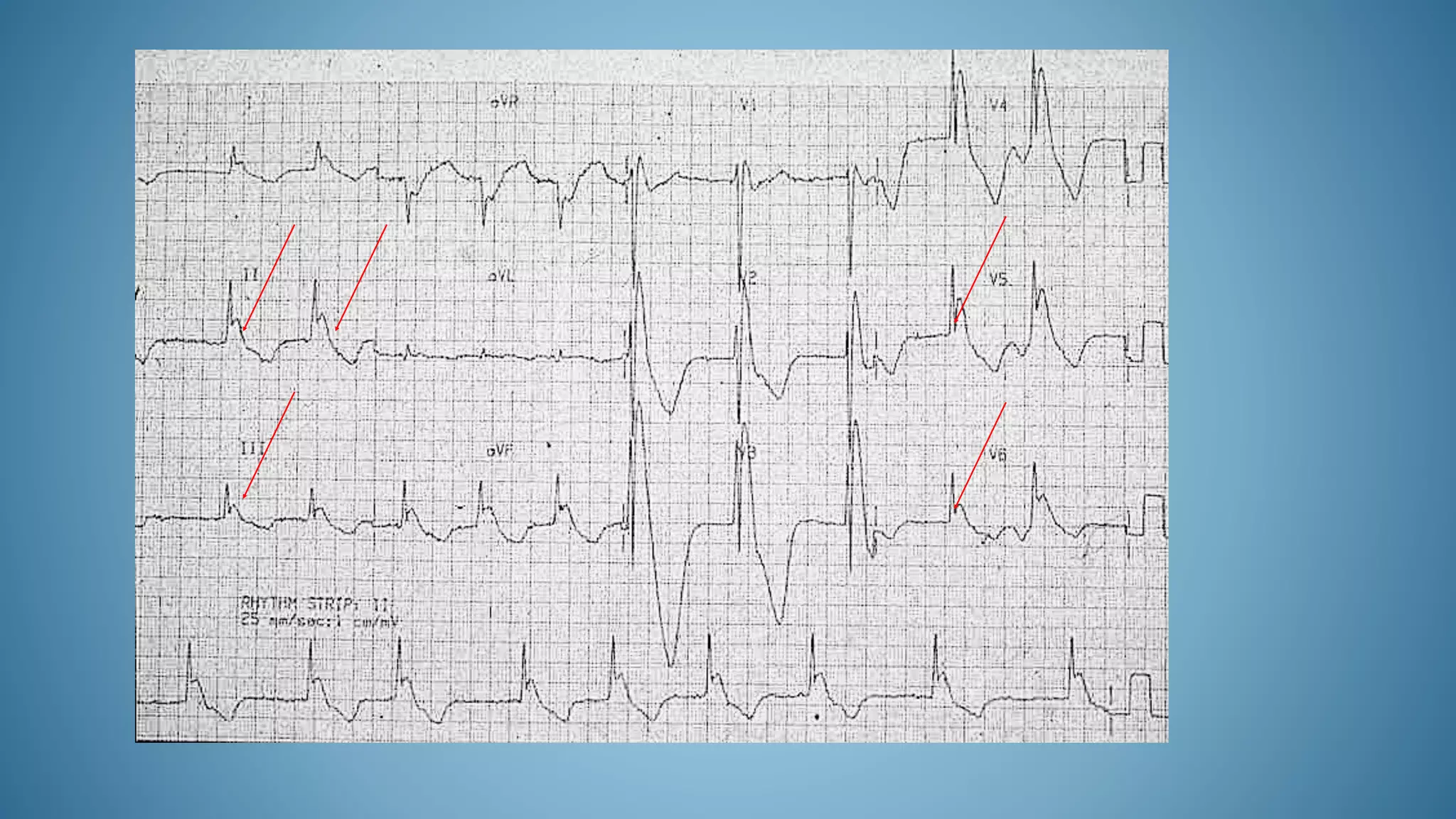
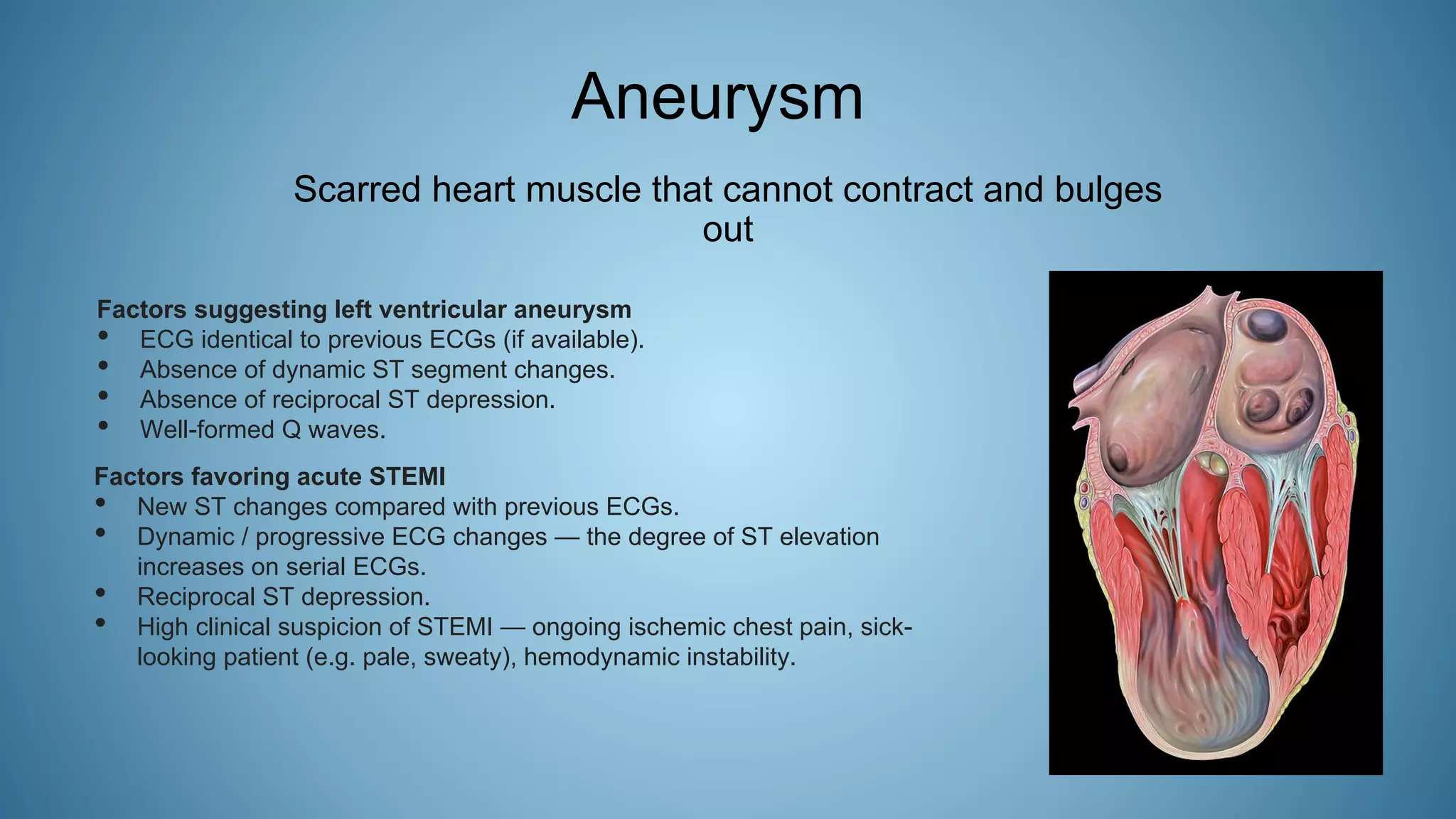
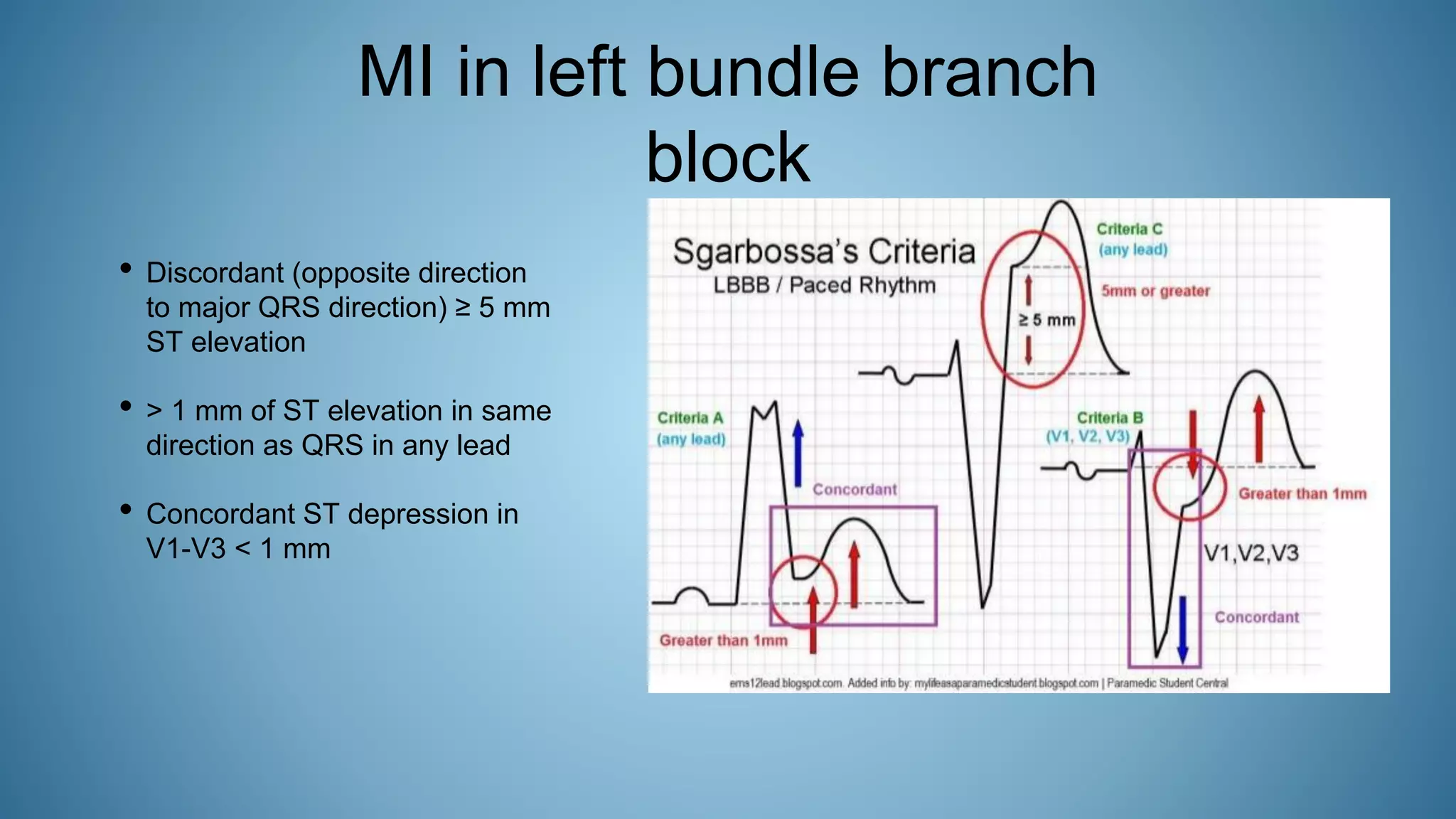
This document summarizes an ECG review presentation given by Dr. Eric Hockstad. It begins with an overview of ECG basics including components like the P wave, PR interval, QRS complex, ST segment, T wave, and QT interval. It then covers various cardiac conditions and how they present on ECG such as heart block, arrhythmias, bundle branch blocks, ST segment changes, and more. Examples are provided of ECGs demonstrating STEMI and cath lab images. Clinical cases are also presented and summarized with ECG findings, treatment outcomes, and teaching points.