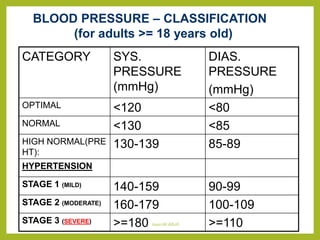
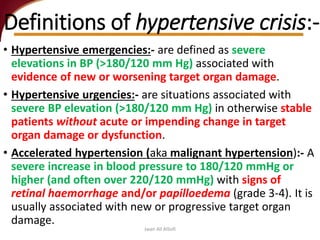
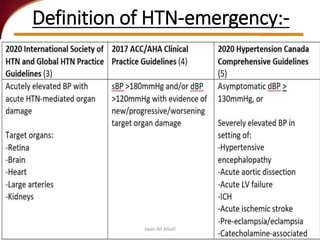
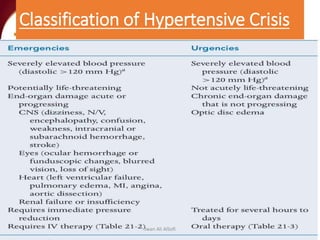
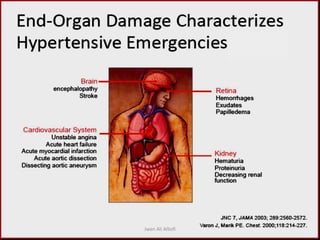
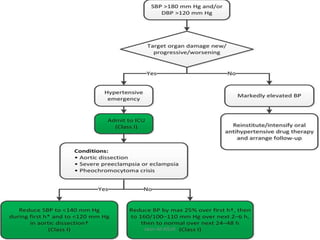
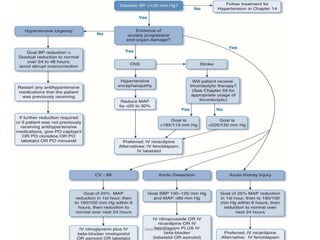
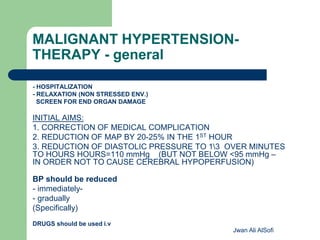
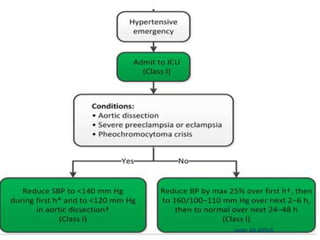
Hypertensive crisis is a condition characterized by a severe elevation in blood pressure, exceeding 180/120 mm Hg, which can be classified into hypertensive emergencies and urgencies based on the presence of target organ damage. It has a low incidence rate but carries significant morbidity and mortality risks, especially among certain demographics. Management focuses on the careful reduction of blood pressure to prevent end-organ damage while maintaining adequate tissue perfusion.