Downloaded 373 times
























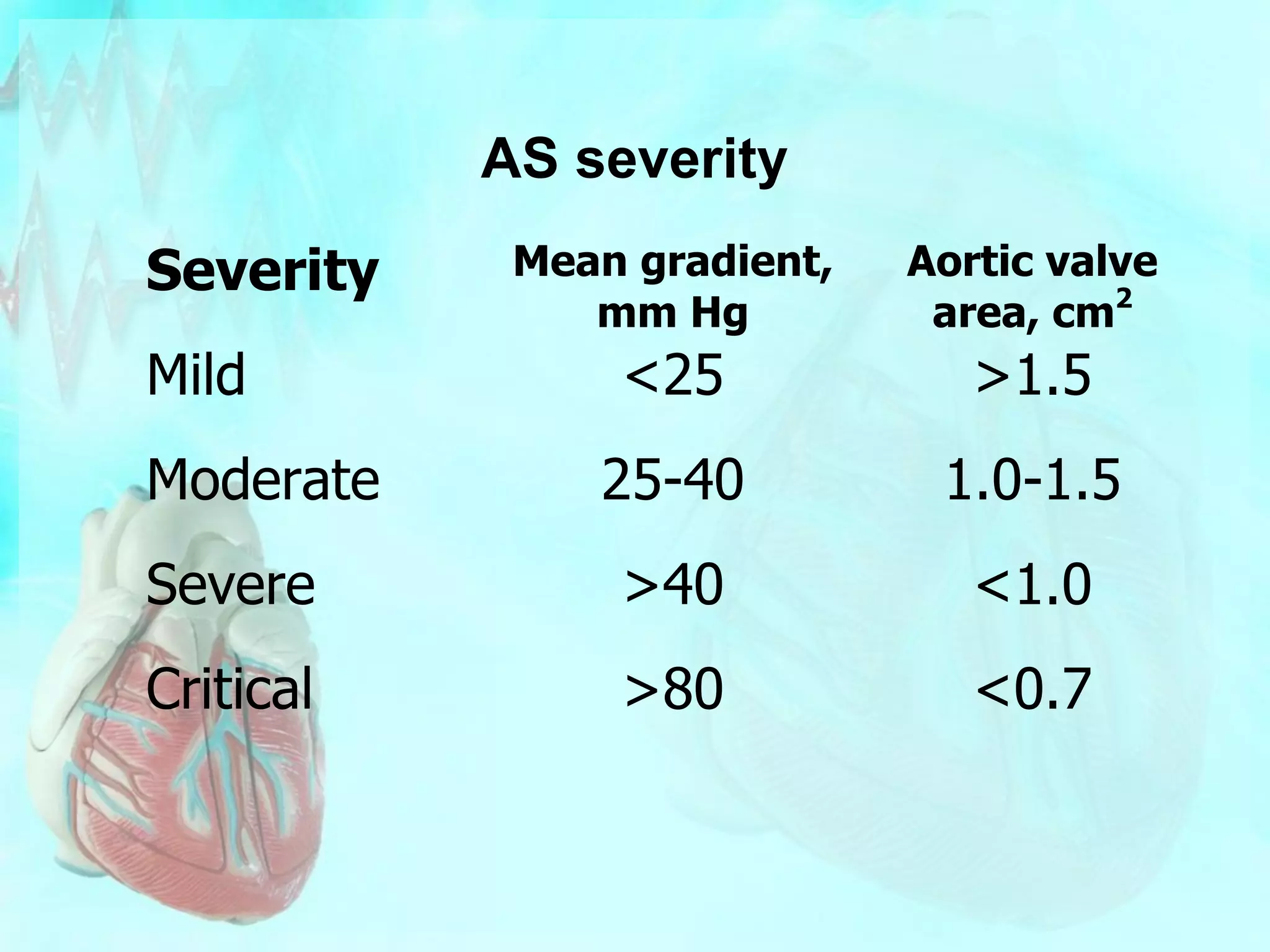












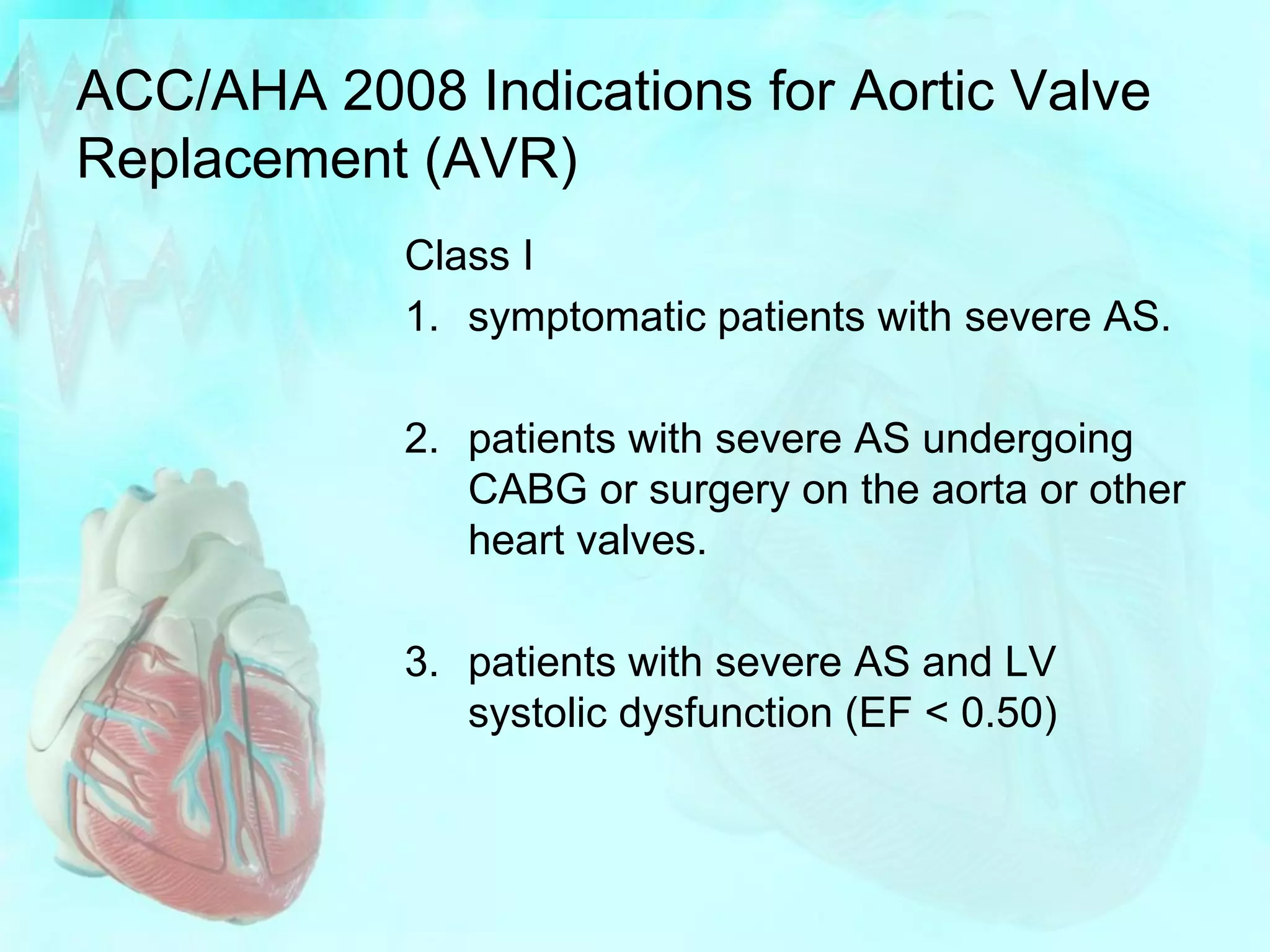


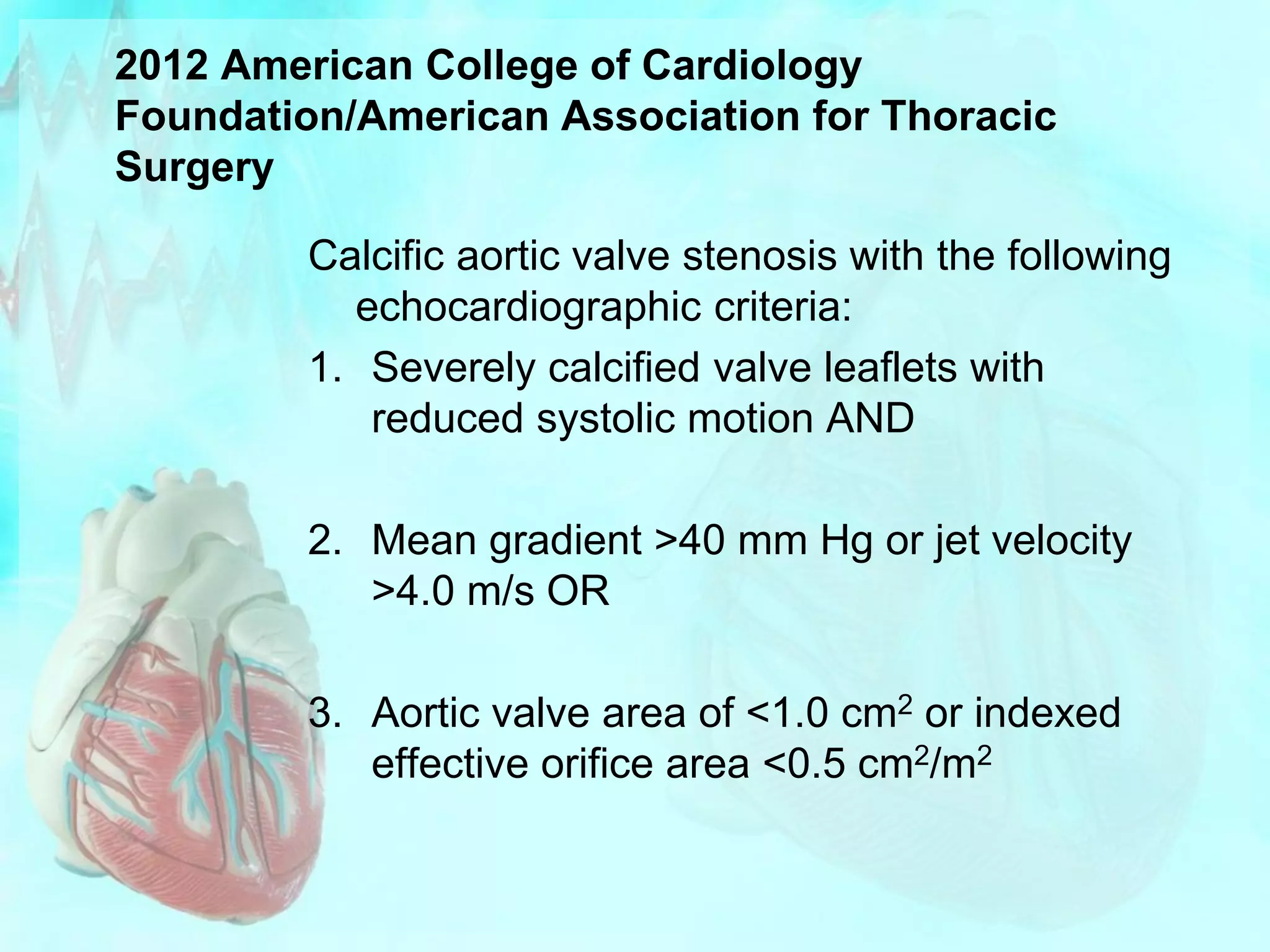



This patient presented with progressive chest pain on exertion and shortness of breath. A physical exam revealed a systolic murmur and echocardiogram showed aortic stenosis with a mean gradient of 32mm Hg and valve area of 0.88cm^2. A cardiac catheterization showed severe aortic stenosis with a peak gradient of 68mm Hg and valve area of 0.83cm^2. Given her symptoms and severity of stenosis, surgical aortic valve replacement is recommended. Coronary angiography will also be performed to assess for need for concomitant CABG prior to surgery.























































































