This document provides information on interpreting EKGs, including:
1. It outlines the 6 main steps to interpret an EKG: identify P waves, measure PR interval, measure QRS complex, identify rhythm, determine heart rate, and interpret strip.
2. It describes common EKG components like the P wave, QRS complex, T wave, and explains how to measure intervals like PR and heart rate.
3. It discusses various arrhythmias and conduction abnormalities like heart blocks, junctional rhythms, atrial fibrillation, and provides characteristics to identify them on an EKG.
crème de la crème basics to understand electrocardiographic analysis in an easy & simple way with some specifications to its use in Emergency medicine/clinical toxicology practice.
crème de la crème basics to understand electrocardiographic analysis in an easy & simple way with some specifications to its use in Emergency medicine/clinical toxicology practice.
Sinus arrhythmia is a normal physiological phenomenon, most commnonly seen in young, healthy people. The heart rate varies due to reflex changes in vagal tone during the different stages of the respiratory cycle. Inspiration increases the heart rate by decreasing vagal tone
ventricular premature complexes and idioventricular rhythm identification is important in the ICU ..they may run into arryhthmias..look over my seminar...
any queries...
ecg basics made easy, with description of most common ecg types especially in emergency situation.
easy to memorize points and mnemonics included.
approach to ecg diagnosis.
sample ecgs.
Sinus arrhythmia is a normal physiological phenomenon, most commnonly seen in young, healthy people. The heart rate varies due to reflex changes in vagal tone during the different stages of the respiratory cycle. Inspiration increases the heart rate by decreasing vagal tone
ventricular premature complexes and idioventricular rhythm identification is important in the ICU ..they may run into arryhthmias..look over my seminar...
any queries...
ecg basics made easy, with description of most common ecg types especially in emergency situation.
easy to memorize points and mnemonics included.
approach to ecg diagnosis.
sample ecgs.
Presentation on basic principles of pediatric ecg with important examples: BY Dr. Nivedita Mishra (PGY2 PEDIATRICS, TRIBHUVAN UNIVERSITY TEACHING HOSPITAL,KATHMANDU,NEPAL)
An electrocardiogram (ECG or EKG) records the electrical signal from your heart to check for different heart conditions. Electrodes are placed on your chest to record your heart's electrical signals, which cause your heart to beat. The signals are shown as waves on an attached computer monitor or printer
ECG Rhythm Interpretation
ST Elevation and non-ST Elevation MIs
ECG Changes
ECG Changes & the Evolving MI
Left Ventricular Hypertrophy
Normal Impulse Conduction
Bundle Branch Blocks
Couples presenting to the infertility clinic- Do they really have infertility...Sujoy Dasgupta
Dr Sujoy Dasgupta presented the study on "Couples presenting to the infertility clinic- Do they really have infertility? – The unexplored stories of non-consummation" in the 13th Congress of the Asia Pacific Initiative on Reproduction (ASPIRE 2024) at Manila on 24 May, 2024.
Recomendações da OMS sobre cuidados maternos e neonatais para uma experiência pós-natal positiva.
Em consonância com os ODS – Objetivos do Desenvolvimento Sustentável e a Estratégia Global para a Saúde das Mulheres, Crianças e Adolescentes, e aplicando uma abordagem baseada nos direitos humanos, os esforços de cuidados pós-natais devem expandir-se para além da cobertura e da simples sobrevivência, de modo a incluir cuidados de qualidade.
Estas diretrizes visam melhorar a qualidade dos cuidados pós-natais essenciais e de rotina prestados às mulheres e aos recém-nascidos, com o objetivo final de melhorar a saúde e o bem-estar materno e neonatal.
Uma “experiência pós-natal positiva” é um resultado importante para todas as mulheres que dão à luz e para os seus recém-nascidos, estabelecendo as bases para a melhoria da saúde e do bem-estar a curto e longo prazo. Uma experiência pós-natal positiva é definida como aquela em que as mulheres, pessoas que gestam, os recém-nascidos, os casais, os pais, os cuidadores e as famílias recebem informação consistente, garantia e apoio de profissionais de saúde motivados; e onde um sistema de saúde flexível e com recursos reconheça as necessidades das mulheres e dos bebês e respeite o seu contexto cultural.
Estas diretrizes consolidadas apresentam algumas recomendações novas e já bem fundamentadas sobre cuidados pós-natais de rotina para mulheres e neonatos que recebem cuidados no pós-parto em unidades de saúde ou na comunidade, independentemente dos recursos disponíveis.
É fornecido um conjunto abrangente de recomendações para cuidados durante o período puerperal, com ênfase nos cuidados essenciais que todas as mulheres e recém-nascidos devem receber, e com a devida atenção à qualidade dos cuidados; isto é, a entrega e a experiência do cuidado recebido. Estas diretrizes atualizam e ampliam as recomendações da OMS de 2014 sobre cuidados pós-natais da mãe e do recém-nascido e complementam as atuais diretrizes da OMS sobre a gestão de complicações pós-natais.
O estabelecimento da amamentação e o manejo das principais intercorrências é contemplada.
Recomendamos muito.
Vamos discutir essas recomendações no nosso curso de pós-graduação em Aleitamento no Instituto Ciclos.
Esta publicação só está disponível em inglês até o momento.
Prof. Marcus Renato de Carvalho
www.agostodourado.com
micro teaching on communication m.sc nursing.pdfAnurag Sharma
Microteaching is a unique model of practice teaching. It is a viable instrument for the. desired change in the teaching behavior or the behavior potential which, in specified types of real. classroom situations, tends to facilitate the achievement of specified types of objectives.
Report Back from SGO 2024: What’s the Latest in Cervical Cancer?bkling
Are you curious about what’s new in cervical cancer research or unsure what the findings mean? Join Dr. Emily Ko, a gynecologic oncologist at Penn Medicine, to learn about the latest updates from the Society of Gynecologic Oncology (SGO) 2024 Annual Meeting on Women’s Cancer. Dr. Ko will discuss what the research presented at the conference means for you and answer your questions about the new developments.
Title: Sense of Taste
Presenter: Dr. Faiza, Assistant Professor of Physiology
Qualifications:
MBBS (Best Graduate, AIMC Lahore)
FCPS Physiology
ICMT, CHPE, DHPE (STMU)
MPH (GC University, Faisalabad)
MBA (Virtual University of Pakistan)
Learning Objectives:
Describe the structure and function of taste buds.
Describe the relationship between the taste threshold and taste index of common substances.
Explain the chemical basis and signal transduction of taste perception for each type of primary taste sensation.
Recognize different abnormalities of taste perception and their causes.
Key Topics:
Significance of Taste Sensation:
Differentiation between pleasant and harmful food
Influence on behavior
Selection of food based on metabolic needs
Receptors of Taste:
Taste buds on the tongue
Influence of sense of smell, texture of food, and pain stimulation (e.g., by pepper)
Primary and Secondary Taste Sensations:
Primary taste sensations: Sweet, Sour, Salty, Bitter, Umami
Chemical basis and signal transduction mechanisms for each taste
Taste Threshold and Index:
Taste threshold values for Sweet (sucrose), Salty (NaCl), Sour (HCl), and Bitter (Quinine)
Taste index relationship: Inversely proportional to taste threshold
Taste Blindness:
Inability to taste certain substances, particularly thiourea compounds
Example: Phenylthiocarbamide
Structure and Function of Taste Buds:
Composition: Epithelial cells, Sustentacular/Supporting cells, Taste cells, Basal cells
Features: Taste pores, Taste hairs/microvilli, and Taste nerve fibers
Location of Taste Buds:
Found in papillae of the tongue (Fungiform, Circumvallate, Foliate)
Also present on the palate, tonsillar pillars, epiglottis, and proximal esophagus
Mechanism of Taste Stimulation:
Interaction of taste substances with receptors on microvilli
Signal transduction pathways for Umami, Sweet, Bitter, Sour, and Salty tastes
Taste Sensitivity and Adaptation:
Decrease in sensitivity with age
Rapid adaptation of taste sensation
Role of Saliva in Taste:
Dissolution of tastants to reach receptors
Washing away the stimulus
Taste Preferences and Aversions:
Mechanisms behind taste preference and aversion
Influence of receptors and neural pathways
Impact of Sensory Nerve Damage:
Degeneration of taste buds if the sensory nerve fiber is cut
Abnormalities of Taste Detection:
Conditions: Ageusia, Hypogeusia, Dysgeusia (parageusia)
Causes: Nerve damage, neurological disorders, infections, poor oral hygiene, adverse drug effects, deficiencies, aging, tobacco use, altered neurotransmitter levels
Neurotransmitters and Taste Threshold:
Effects of serotonin (5-HT) and norepinephrine (NE) on taste sensitivity
Supertasters:
25% of the population with heightened sensitivity to taste, especially bitterness
Increased number of fungiform papillae
These simplified slides by Dr. Sidra Arshad present an overview of the non-respiratory functions of the respiratory tract.
Learning objectives:
1. Enlist the non-respiratory functions of the respiratory tract
2. Briefly explain how these functions are carried out
3. Discuss the significance of dead space
4. Differentiate between minute ventilation and alveolar ventilation
5. Describe the cough and sneeze reflexes
Study Resources:
1. Chapter 39, Guyton and Hall Textbook of Medical Physiology, 14th edition
2. Chapter 34, Ganong’s Review of Medical Physiology, 26th edition
3. Chapter 17, Human Physiology by Lauralee Sherwood, 9th edition
4. Non-respiratory functions of the lungs https://academic.oup.com/bjaed/article/13/3/98/278874
HOT NEW PRODUCT! BIG SALES FAST SHIPPING NOW FROM CHINA!! EU KU DB BK substit...GL Anaacs
Contact us if you are interested:
Email / Skype : kefaya1771@gmail.com
Threema: PXHY5PDH
New BATCH Ku !!! MUCH IN DEMAND FAST SALE EVERY BATCH HAPPY GOOD EFFECT BIG BATCH !
Contact me on Threema or skype to start big business!!
Hot-sale products:
NEW HOT EUTYLONE WHITE CRYSTAL!!
5cl-adba precursor (semi finished )
5cl-adba raw materials
ADBB precursor (semi finished )
ADBB raw materials
APVP powder
5fadb/4f-adb
Jwh018 / Jwh210
Eutylone crystal
Protonitazene (hydrochloride) CAS: 119276-01-6
Flubrotizolam CAS: 57801-95-3
Metonitazene CAS: 14680-51-4
Payment terms: Western Union,MoneyGram,Bitcoin or USDT.
Deliver Time: Usually 7-15days
Shipping method: FedEx, TNT, DHL,UPS etc.Our deliveries are 100% safe, fast, reliable and discreet.
Samples will be sent for your evaluation!If you are interested in, please contact me, let's talk details.
We specializes in exporting high quality Research chemical, medical intermediate, Pharmaceutical chemicals and so on. Products are exported to USA, Canada, France, Korea, Japan,Russia, Southeast Asia and other countries.
Knee anatomy and clinical tests 2024.pdfvimalpl1234
This includes all relevant anatomy and clinical tests compiled from standard textbooks, Campbell,netter etc..It is comprehensive and best suited for orthopaedicians and orthopaedic residents.
NVBDCP.pptx Nation vector borne disease control programSapna Thakur
NVBDCP was launched in 2003-2004 . Vector-Borne Disease: Disease that results from an infection transmitted to humans and other animals by blood-feeding arthropods, such as mosquitoes, ticks, and fleas. Examples of vector-borne diseases include Dengue fever, West Nile Virus, Lyme disease, and malaria.
Explore natural remedies for syphilis treatment in Singapore. Discover alternative therapies, herbal remedies, and lifestyle changes that may complement conventional treatments. Learn about holistic approaches to managing syphilis symptoms and supporting overall health.
Title: Sense of Smell
Presenter: Dr. Faiza, Assistant Professor of Physiology
Qualifications:
MBBS (Best Graduate, AIMC Lahore)
FCPS Physiology
ICMT, CHPE, DHPE (STMU)
MPH (GC University, Faisalabad)
MBA (Virtual University of Pakistan)
Learning Objectives:
Describe the primary categories of smells and the concept of odor blindness.
Explain the structure and location of the olfactory membrane and mucosa, including the types and roles of cells involved in olfaction.
Describe the pathway and mechanisms of olfactory signal transmission from the olfactory receptors to the brain.
Illustrate the biochemical cascade triggered by odorant binding to olfactory receptors, including the role of G-proteins and second messengers in generating an action potential.
Identify different types of olfactory disorders such as anosmia, hyposmia, hyperosmia, and dysosmia, including their potential causes.
Key Topics:
Olfactory Genes:
3% of the human genome accounts for olfactory genes.
400 genes for odorant receptors.
Olfactory Membrane:
Located in the superior part of the nasal cavity.
Medially: Folds downward along the superior septum.
Laterally: Folds over the superior turbinate and upper surface of the middle turbinate.
Total surface area: 5-10 square centimeters.
Olfactory Mucosa:
Olfactory Cells: Bipolar nerve cells derived from the CNS (100 million), with 4-25 olfactory cilia per cell.
Sustentacular Cells: Produce mucus and maintain ionic and molecular environment.
Basal Cells: Replace worn-out olfactory cells with an average lifespan of 1-2 months.
Bowman’s Gland: Secretes mucus.
Stimulation of Olfactory Cells:
Odorant dissolves in mucus and attaches to receptors on olfactory cilia.
Involves a cascade effect through G-proteins and second messengers, leading to depolarization and action potential generation in the olfactory nerve.
Quality of a Good Odorant:
Small (3-20 Carbon atoms), volatile, water-soluble, and lipid-soluble.
Facilitated by odorant-binding proteins in mucus.
Membrane Potential and Action Potential:
Resting membrane potential: -55mV.
Action potential frequency in the olfactory nerve increases with odorant strength.
Adaptation Towards the Sense of Smell:
Rapid adaptation within the first second, with further slow adaptation.
Psychological adaptation greater than receptor adaptation, involving feedback inhibition from the central nervous system.
Primary Sensations of Smell:
Camphoraceous, Musky, Floral, Pepperminty, Ethereal, Pungent, Putrid.
Odor Detection Threshold:
Examples: Hydrogen sulfide (0.0005 ppm), Methyl-mercaptan (0.002 ppm).
Some toxic substances are odorless at lethal concentrations.
Characteristics of Smell:
Odor blindness for single substances due to lack of appropriate receptor protein.
Behavioral and emotional influences of smell.
Transmission of Olfactory Signals:
From olfactory cells to glomeruli in the olfactory bulb, involving lateral inhibition.
Primitive, less old, and new olfactory systems with different path
Flu Vaccine Alert in Bangalore Karnatakaaddon Scans
As flu season approaches, health officials in Bangalore, Karnataka, are urging residents to get their flu vaccinations. The seasonal flu, while common, can lead to severe health complications, particularly for vulnerable populations such as young children, the elderly, and those with underlying health conditions.
Dr. Vidisha Kumari, a leading epidemiologist in Bangalore, emphasizes the importance of getting vaccinated. "The flu vaccine is our best defense against the influenza virus. It not only protects individuals but also helps prevent the spread of the virus in our communities," he says.
This year, the flu season is expected to coincide with a potential increase in other respiratory illnesses. The Karnataka Health Department has launched an awareness campaign highlighting the significance of flu vaccinations. They have set up multiple vaccination centers across Bangalore, making it convenient for residents to receive their shots.
To encourage widespread vaccination, the government is also collaborating with local schools, workplaces, and community centers to facilitate vaccination drives. Special attention is being given to ensuring that the vaccine is accessible to all, including marginalized communities who may have limited access to healthcare.
Residents are reminded that the flu vaccine is safe and effective. Common side effects are mild and may include soreness at the injection site, mild fever, or muscle aches. These side effects are generally short-lived and far less severe than the flu itself.
Healthcare providers are also stressing the importance of continuing COVID-19 precautions. Wearing masks, practicing good hand hygiene, and maintaining social distancing are still crucial, especially in crowded places.
Protect yourself and your loved ones by getting vaccinated. Together, we can help keep Bangalore healthy and safe this flu season. For more information on vaccination centers and schedules, residents can visit the Karnataka Health Department’s official website or follow their social media pages.
Stay informed, stay safe, and get your flu shot today!
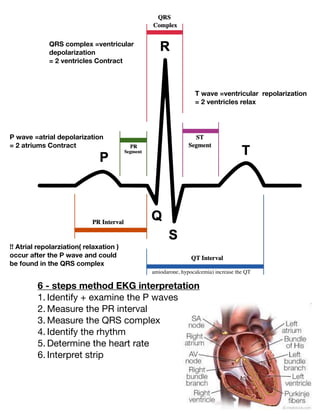
1. 6 - steps method EKG interpretation
1. Identify + examine the P waves
2. Measure the PR interval
3. Measure the QRS complex
4. Identify the rhythm
5. Determine the heart rate
6. Interpret strip
P wave =atrial depolarization
= 2 atriums Contract
QRS complex =ventricular
depolarization
= 2 ventricles Contract
T wave =ventricular repolarization
= 2 ventricles relax
!! Atrial repolarziation( relaxation )
occur after the P wave and could
be found in the QRS complex
amiodarone, hypocalcemia) increase the QT
2. P wave = should be present and upright
Inverted = junctional rhythm
Absent = ventricular
fi
brillation
PR interval = distance between P wave and the beginning of QRS
complex . What we do ??
We count the number of small boxes in between and multiply it by
0.04 seconds
!! Normal PR should be 0.12-0.20
> 0.20 = heart blocks
QRS complex: measure the small boxes in between the QRS
!! Normal = 0.08-0.12
>0.12 = PVC “ Premature ventricular contractions”
To identify the rhythm: measure the distance between R …R
Distance should be the same otherwise they will be
Irregular.
Heart rate :
1) 6 second method
Only If there are these lines then this is EKG is a 6 second strip
From the
fi
rst line to the third = 6 second strip
So we do 6 second method : we count the number of R between
these 3 lines and multiply by 10
Example this
fi
gure above: we have 6 R … 6*10= 60 Heart beat/min
!! Left atrial (LA) abnormality may cause broad, often
notched P waves in the limb leads and a biphasic P
wave in lead V1
3. INFO:
ABG “arterial blood gases”
= measurements of acidity and alkalinity of the arterial
circulation+ measure gases( ex: oxygen + carbon dioxide)
4 main components of ABG = PH + CO2+ HCO3
“bicarbonate” + PaO2”oxygen”
Heart blocks
May be found between SA node and the AV node or between
the AV node and the bundle of his to the purkinjie
fi
bers .
Causes : scarring of cardiac cells due to aging , heart attacks
, valve infections by endocarditis / medications “ex: digoxin”.
4 Types :
1. First degree heart block : partial block between the sa
node and the av node .
EKG: consistent prolonged PR interval ( measure the small
boxes of PRI and multiply by 0,04)
2) big box method
Divide 300 by the number of big boxes between 2 R
300/5 =60 BPM
4. 2. second degree heart block type 1”wenckebach”
Progressive block between av and sa node
ECG: begin with normal PRI then Progressive longer PRI
then dropped QRS .
!! Longer PRI is because of the delay from the conduction
from sa node to purkinje
fi
bers
3. second degree heart block type 2 / mobitz II
Intermittent block between sa and av node , block is complete
not partial.
ECG: drop in
QRS complex
+constant PR
interval
4. third degree heart block
” Complete heart block “+ bradycardic rhythm
ECG: no correlation between P waves and QRS complex
P waves have the same distance also QRS has same distance ,
but there is no correlation … p waves occur because atriums are
contracting ….and QRS occur because ventricles are
contracting, but they are independent .
5. Junctional Rhythms
Here the SA node fails / it has weak impulse…. Then the AV node will take
place and generate it’s own impulse…. That makes the typical junctional
heart rhythm= 40-60/min.
Characteristics :
1. HR 40-60 bpm
2. P wave is inverted / absent … also there may be a “ retrograde
impulse” where the inverted P wave goes after the QRS complex
Classi
fi
cation :
Junctional rhythm 40-60 bpm
Accelerated Junctional rhythm 60-100 bpm
Junctional tachycardia >100 bpm
Junctional Bradycardia < 40 bpm
!! The only thing that di
ff
erentiate between them is the heart rate ,,,, and
has one thing in common which is that the P wave is inverted /absent .
! Other Classi
fi
cation
Premature junctional complex (PJC)
Wandering junctional pacemaker dysrhthmyia
P wave -retrograde
6. Atrial
fi
brillation + Atrial Flutter
In atrial
fi
brillation:
Instead of having just the SA node conducting the
fi
rst
impulse toward the AV node … we will have several
cardiac cells in atriums ,,, they conduct their own impulse
with the SA node causing both atriums to contract much
faster than normal .
Characteristics :
1.“Regularly irregular rhythm “= distance between R
intervals will be di
ff
erent
2. No de
fi
nite P-waves
We call these in circles “ quiver waves
Types
Determined by the HR …
if 60-100 bpm = controlled atrial
fi
brillation
If < 60 bpm = atrial
fi
brillation with slow ventricular
response
If 101-150 = atrial
fi
brillation with rapid ventricular
response
If > 150 bpm = uncontrolled atrial
fi
brillation
In Atrial
fl
utter :
There is only one extra cardiac cell on top of SA node
either in left or right atrium.
-Saw-tooth waves
-Regular rhythm
7. Chest Leads
v1-v6”
precordial
leads”
The chest leads look at the heart in a horizontal
plane
V1 the right most view and V6 the left most .
!! In normal conduction, depolarization of the septum
starts from the left bundle going to the right toward v1
away from v6 , the left ventricle is larger so
the movement is to the left away from v1 to
v6 .
This causes negative wave in V 1 and
positive wave in v6.
—From v3-v4 it is isoelectric with
similar pos + neg de
fl
ections ..known as
transitional zone .
If transition happens in V2 = early transition/
rightward shift / counterclockwise
rotation .
2
ty
pes of leads
1) six chest leads v1-v6 ( examine the
fl
ow of depolarization
and repolarization of the heart in horizontal plane )
2) frontal leads ( examine the electrical events in verticalplane)
8. If it happened after V4 = late transition /
leftward shift / clockwise rotation
Causes may be : incorrect placement of
electrodes ( too low /high) / Anatomical
variations
— increase in R wave from V1-V5 known as
R wave progression
!! clockwise rotation more likely pathological
Example : COPD , anterior myocardial infarction ,
dilated cardiomyopathy
!! counterclockwise rotation more common in healthy
individual
Clinical causes ex: condition problems “ posterior MI”
Electrical shift to the right “RVH”
!! If transitional zone is absent / unclear = pathological
In this case we look at the R wave progression ,,, non/
poor progression …R wave stay low and S wave
remains deep in all chest leads = extensive anterior MI
— reverse progression of R wave ,,tall Wave in V1 /v2=
seen in right ventricular hypertrophy ( because
increased muscle mass in the right ventricle result in
net electrical movement toward the right chest leads.
10. !!! These groups of leads do not only analyze
cardiac electrical events in the anatomical area
indicated
lead V1 : fourth intercostal space to the right of the sternum
lead V2: fourth intercostal space, just to the left of thesternum
lead V3 : midway between V2 and V4; lead V4, midclavicular line,
fi
fth intercostal
space
lead V5 : anterior axillary line, same level as V4
lead V6 :midaxillary line, same level as V4 and V5. A
11. Myocardial infarction
ECG (during / following MI ) :
1.Pathological Q waves
2.New QRS axis deviation
3.Poor R wave progression
4.Conduction block “AV block, bundle
branch block )