Downloaded 319 times
![[ECG] APPROACH TO[ECG] APPROACH TO
ARRHYTHMIASARRHYTHMIAS
(WITH ELECTROPHYSIOLOGICAL PERSPECTIVES)(WITH ELECTROPHYSIOLOGICAL PERSPECTIVES)
Dr. ASHUTOSH](https://image.slidesharecdn.com/ecgapproachtoarrhythmias2017-180424151935/75/ECG-approach-to-arrhythmias-2017-1-2048.jpg)



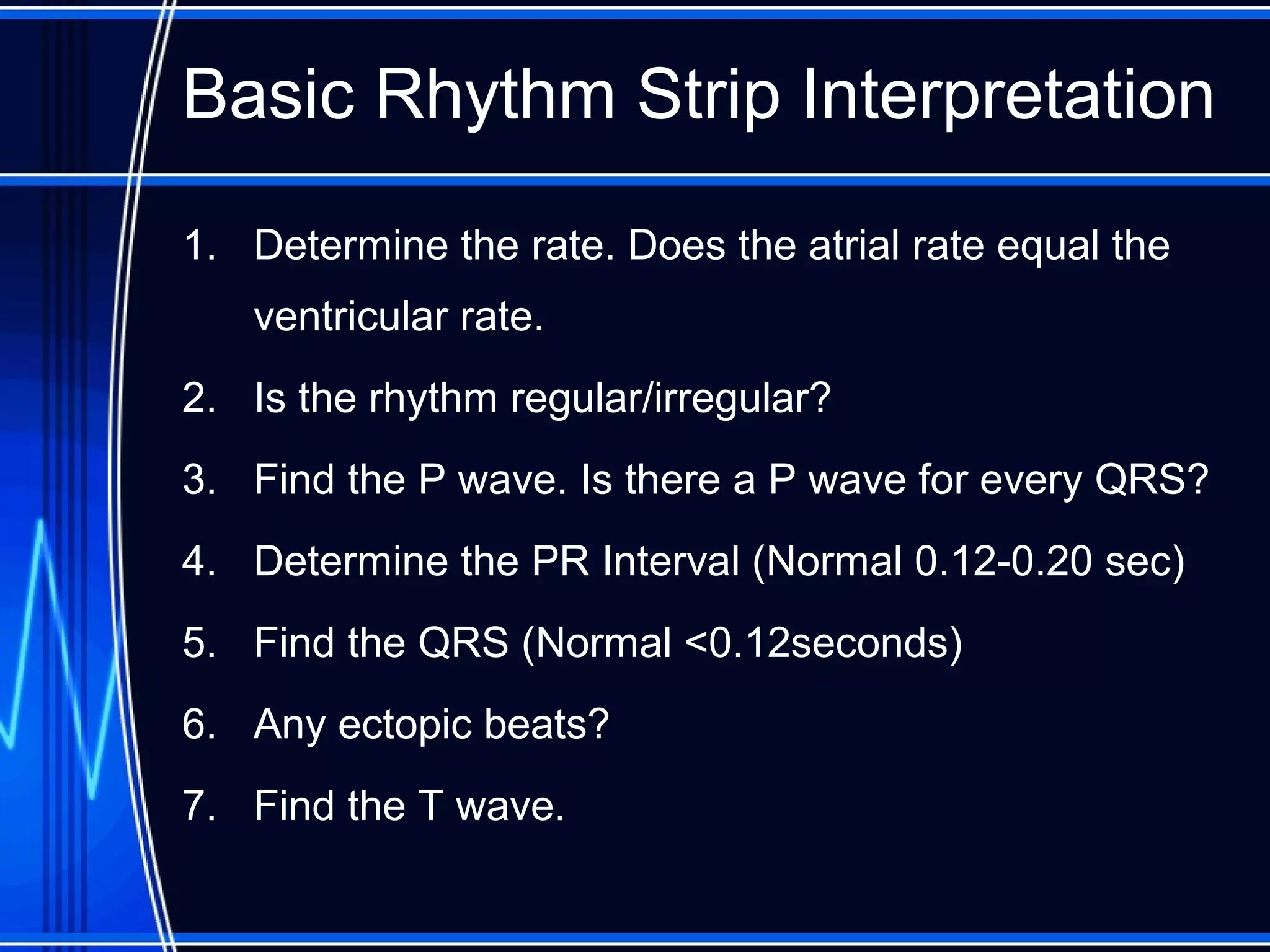



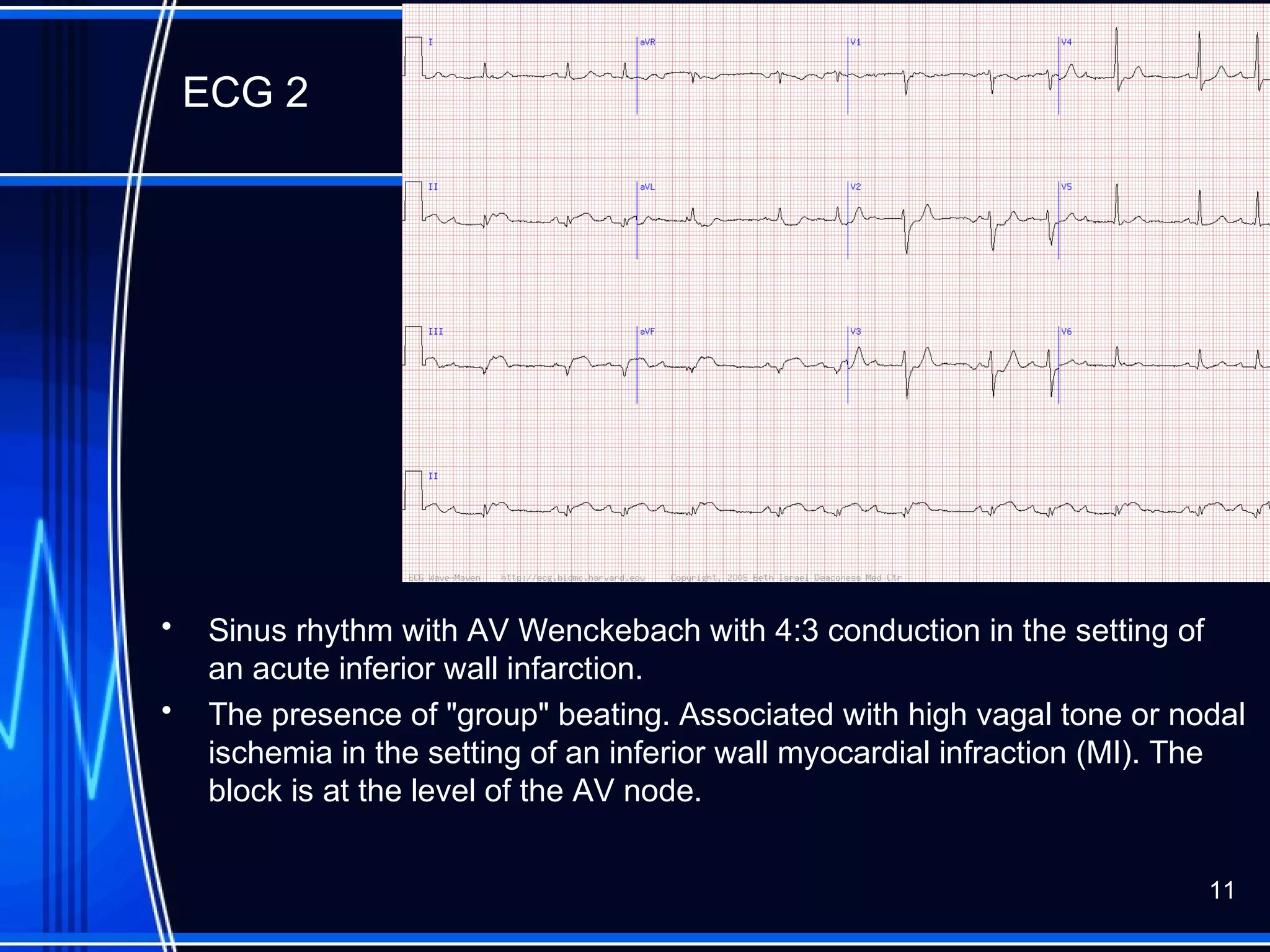


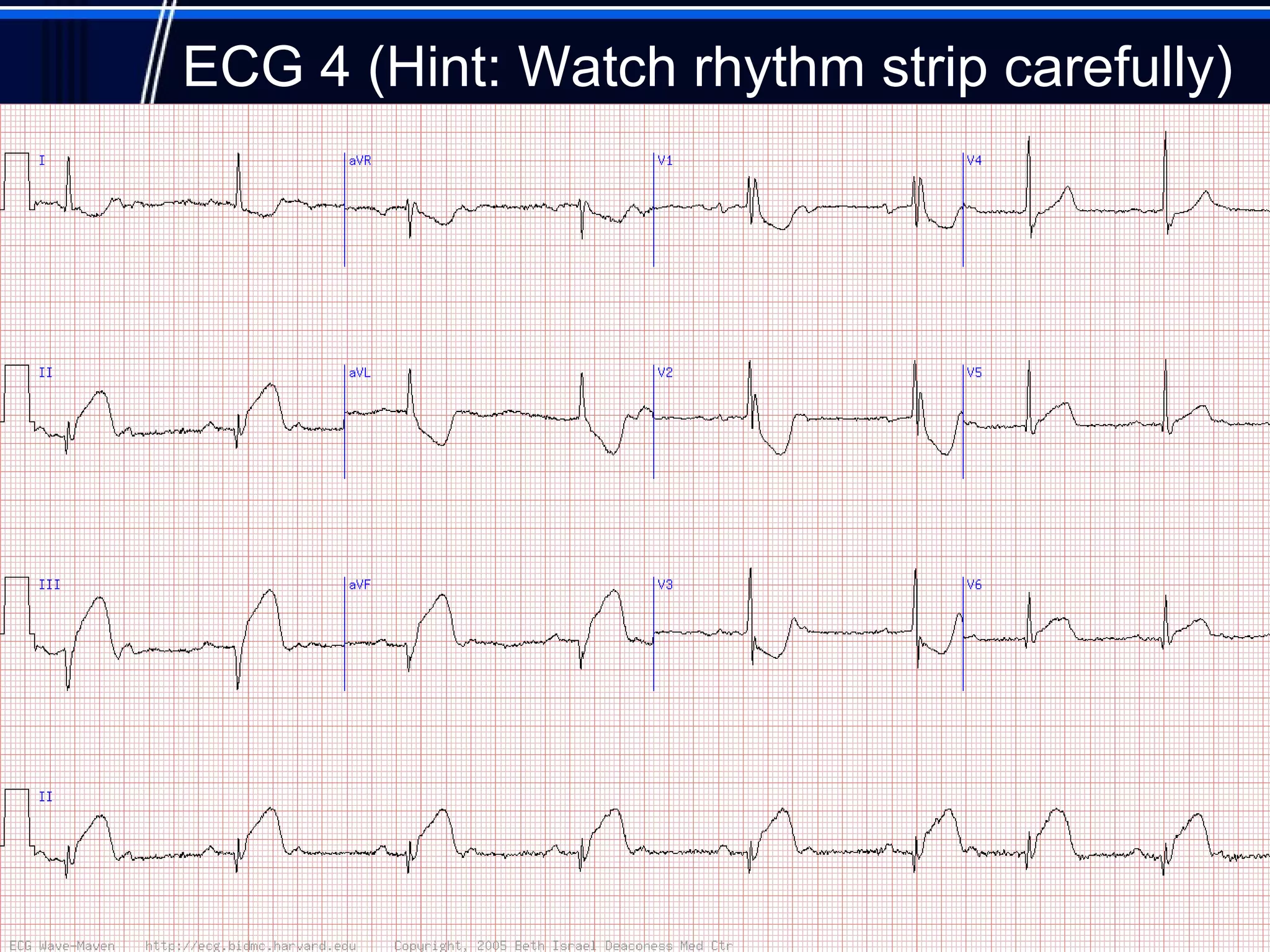

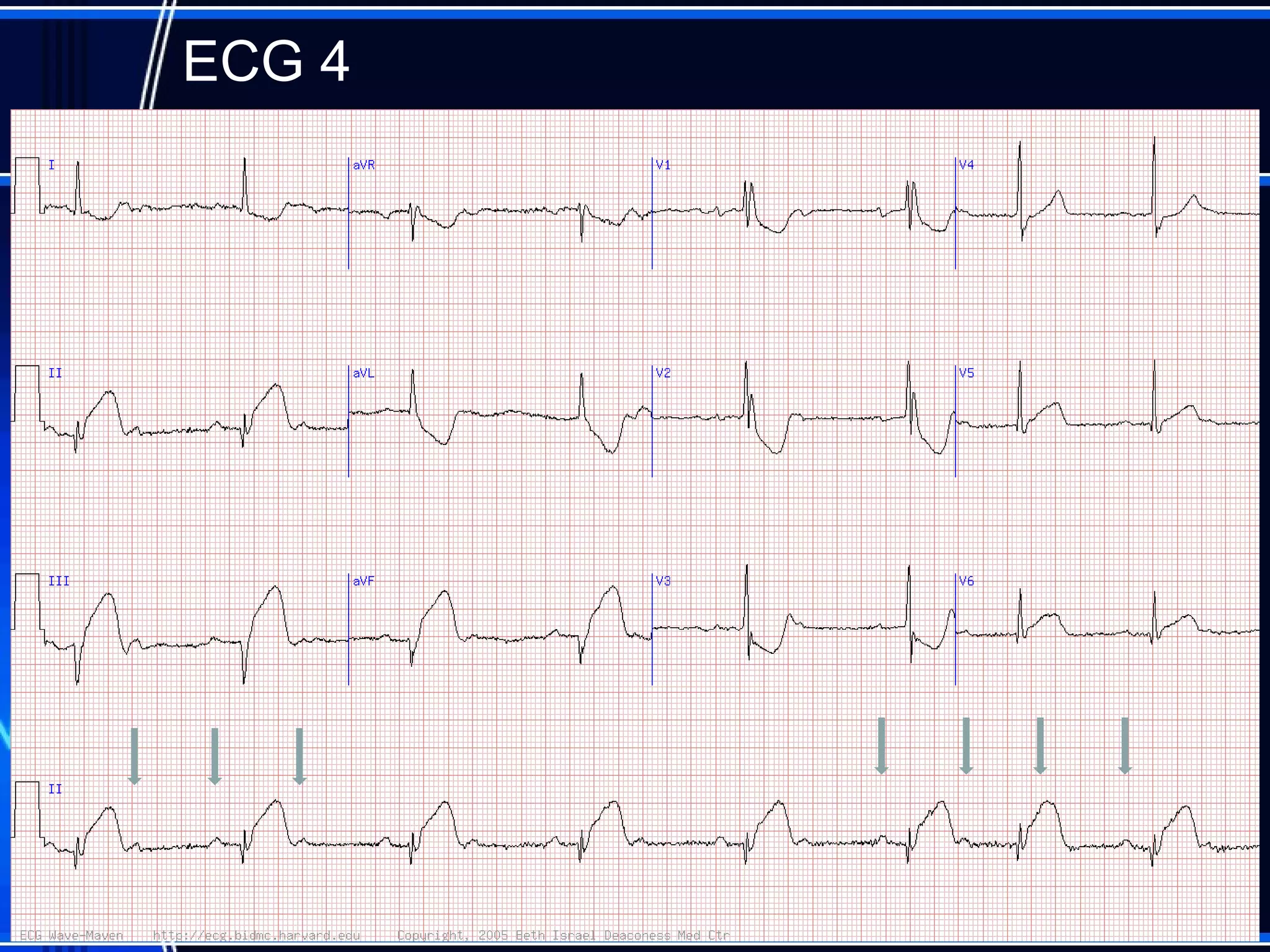
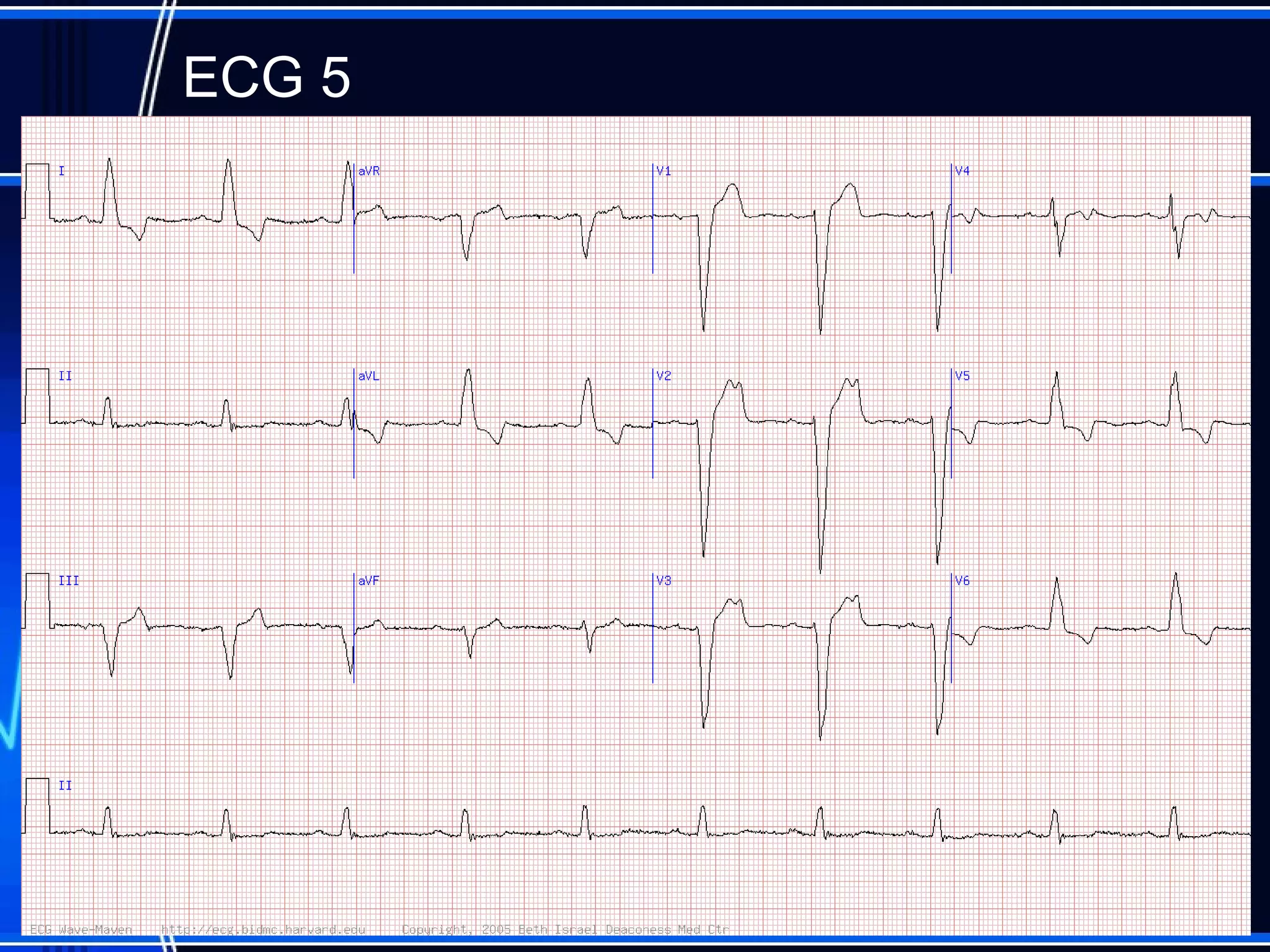











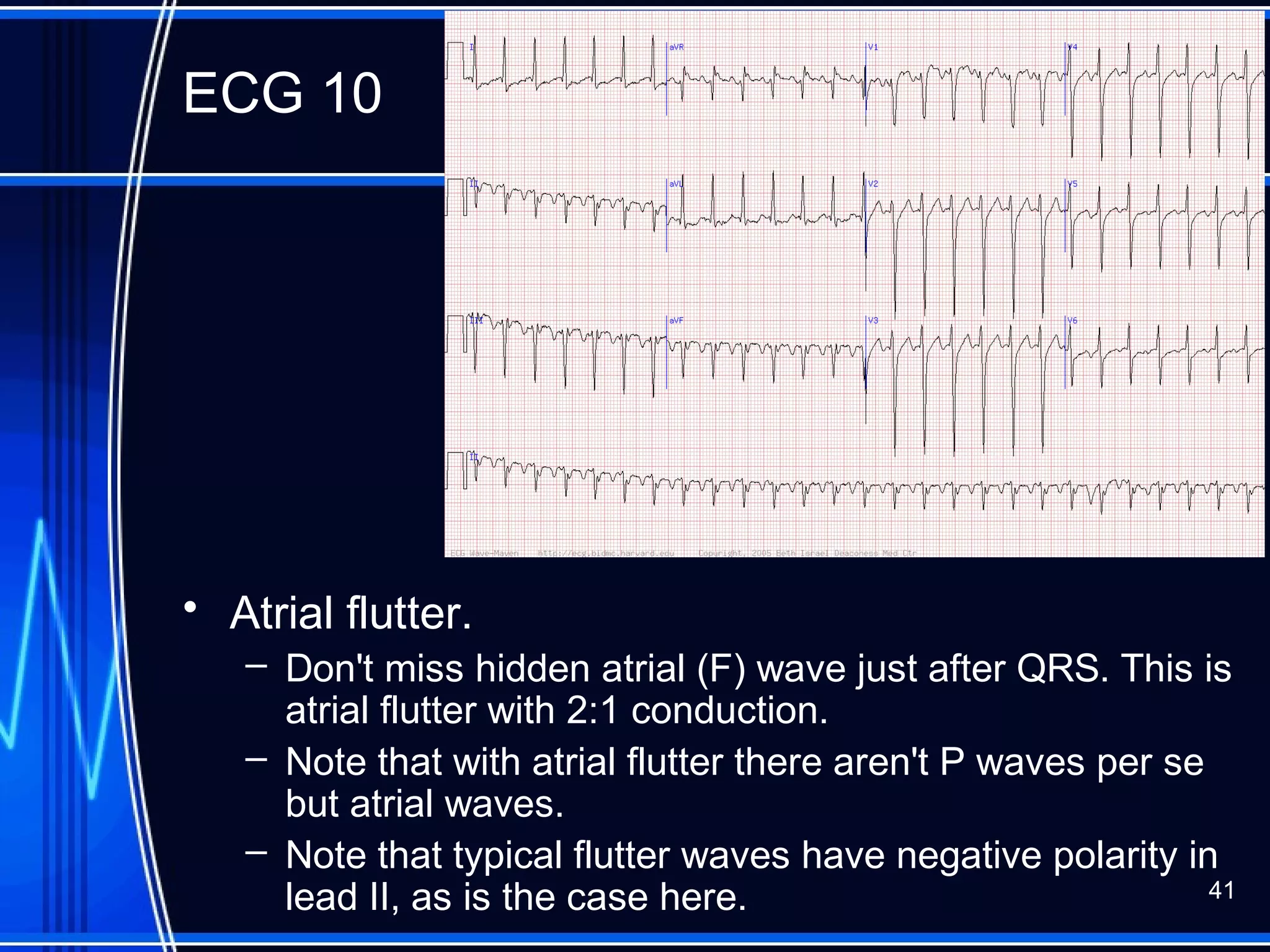

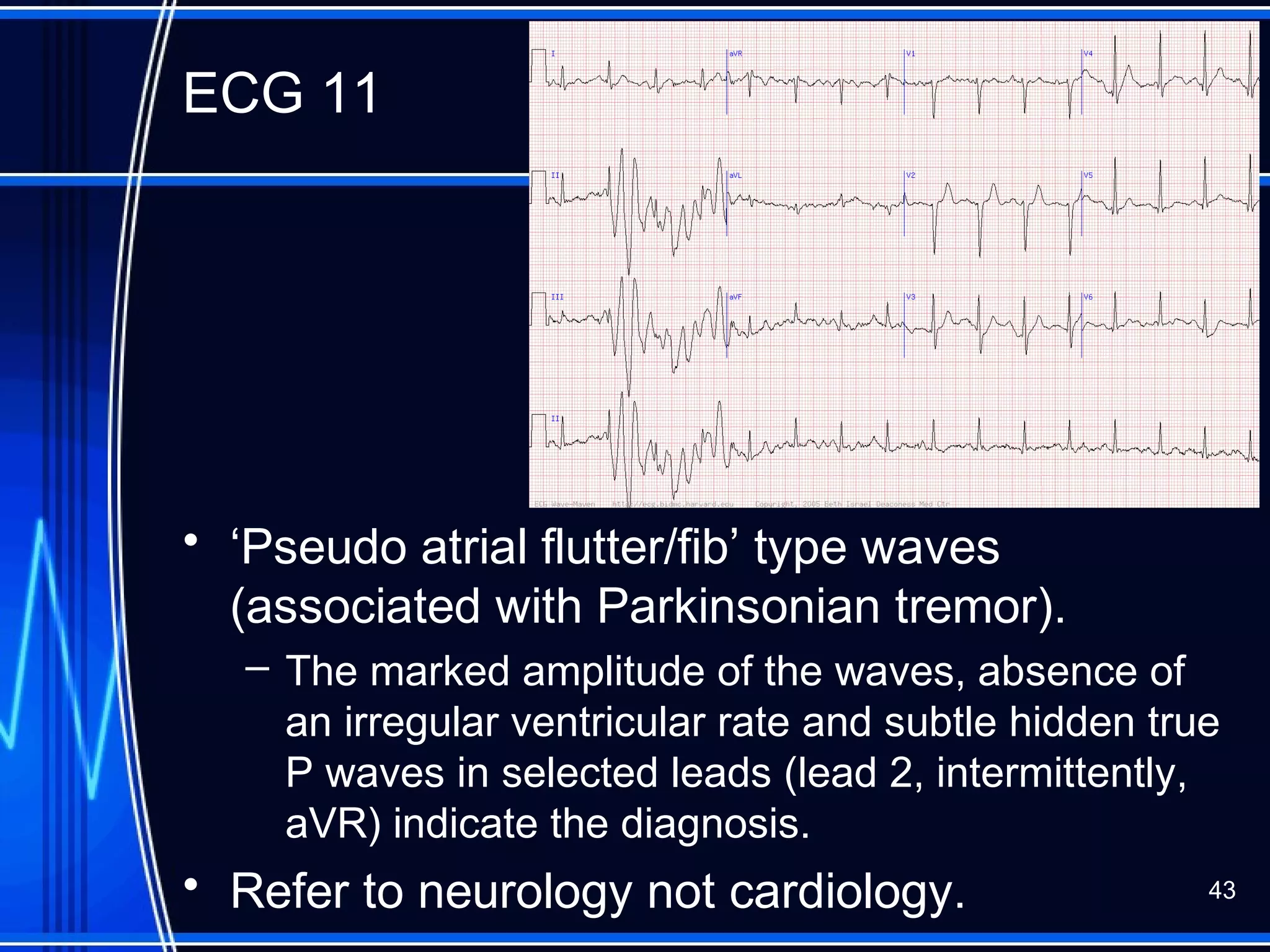
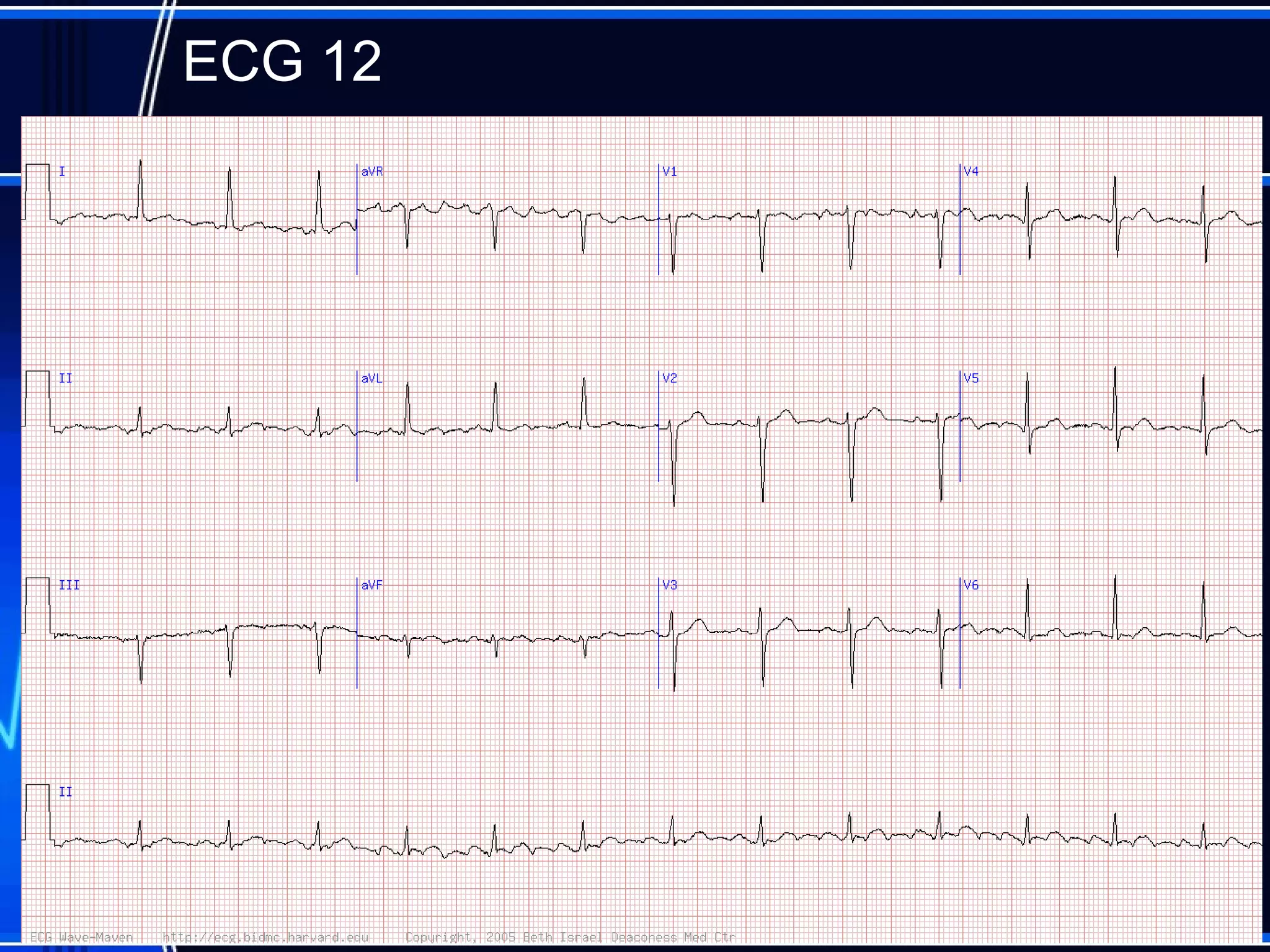

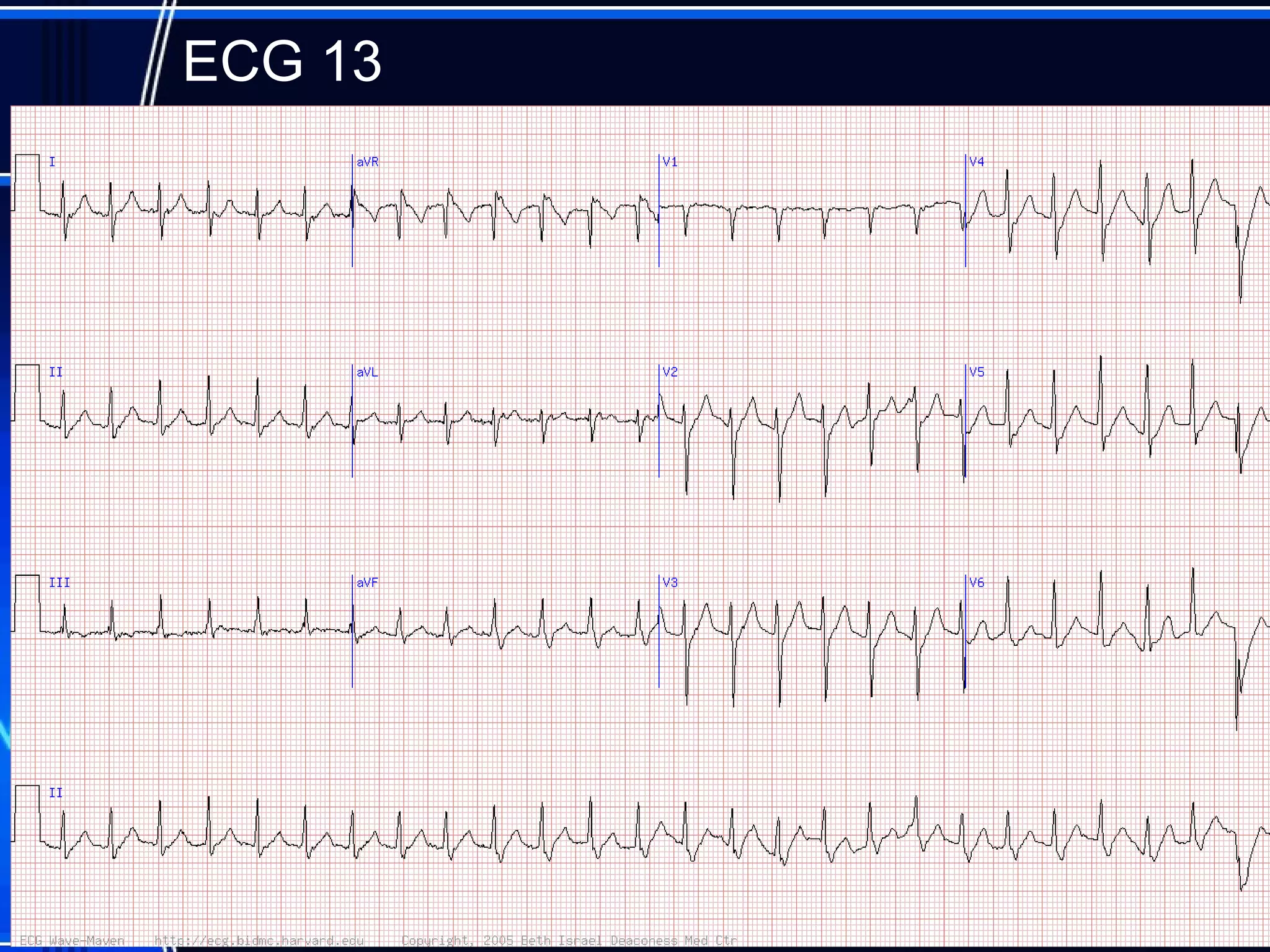

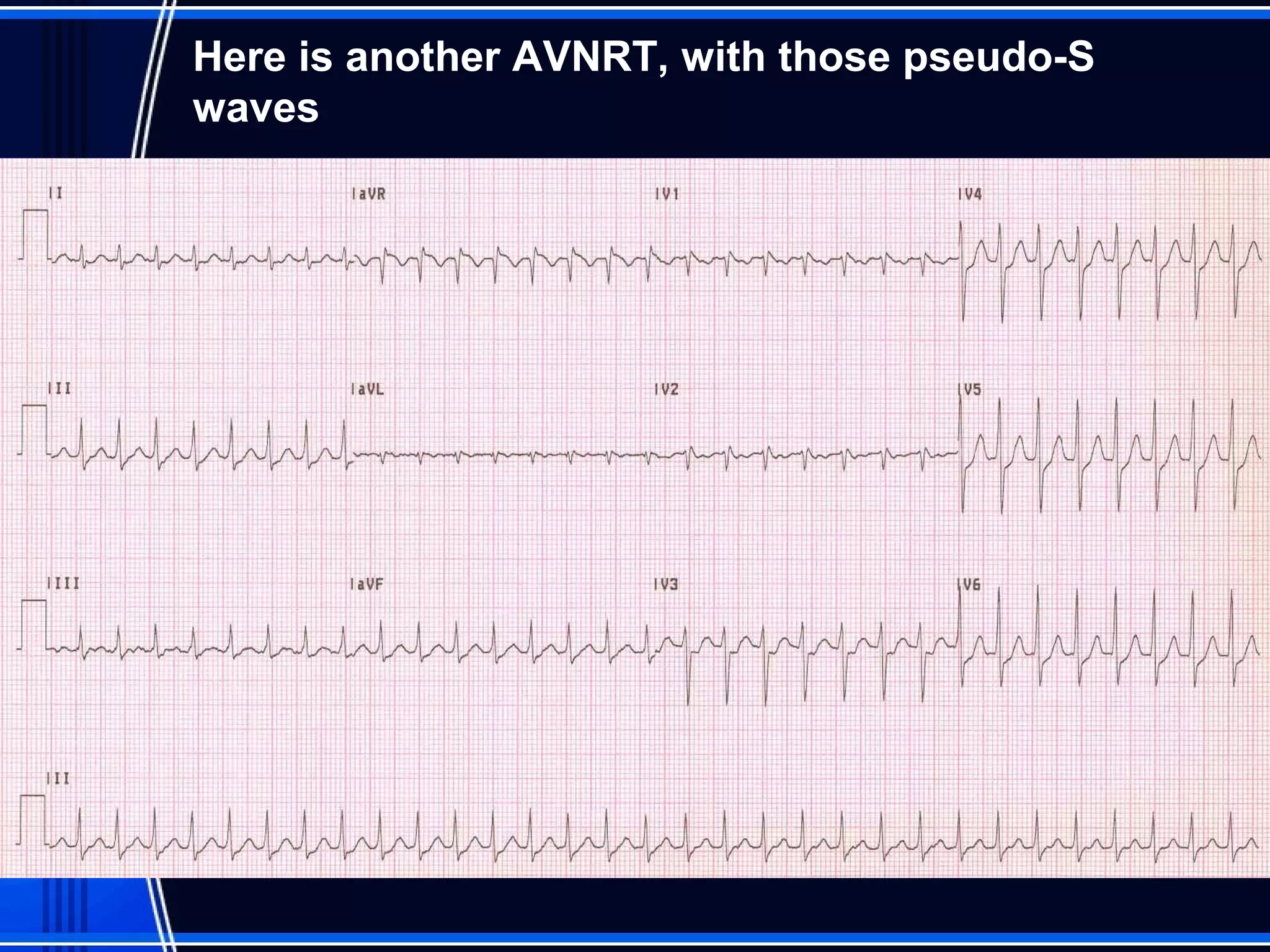
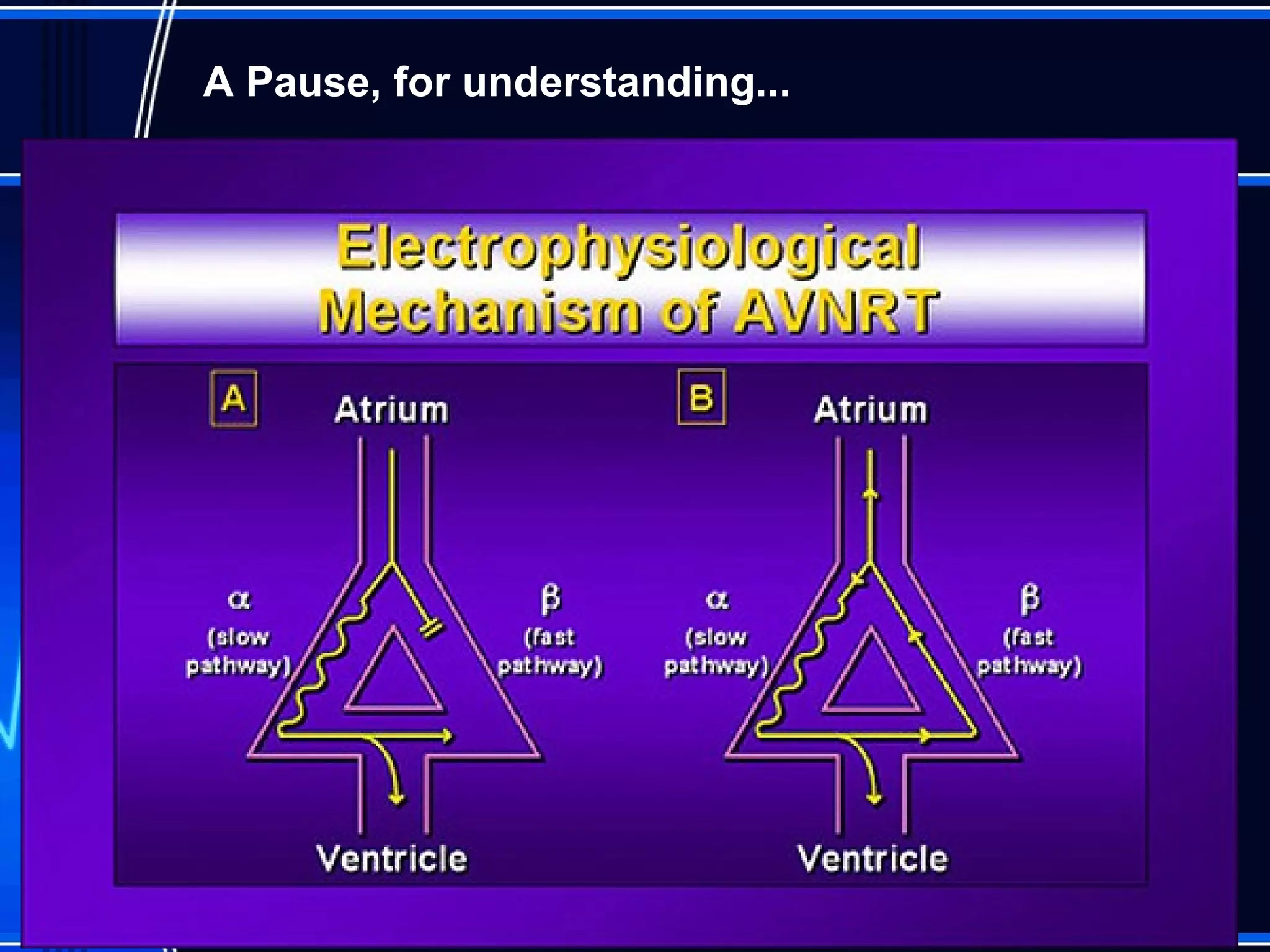
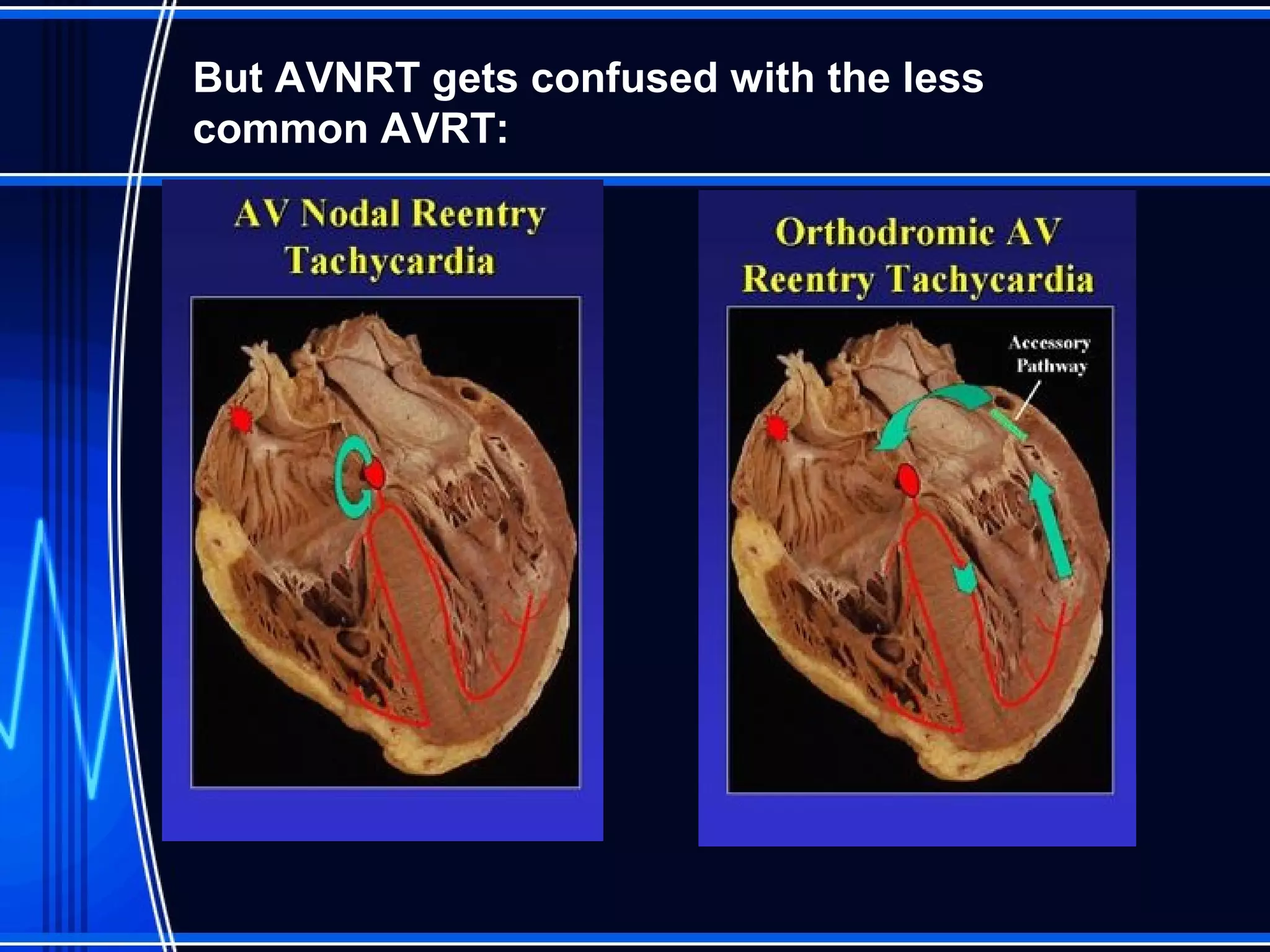

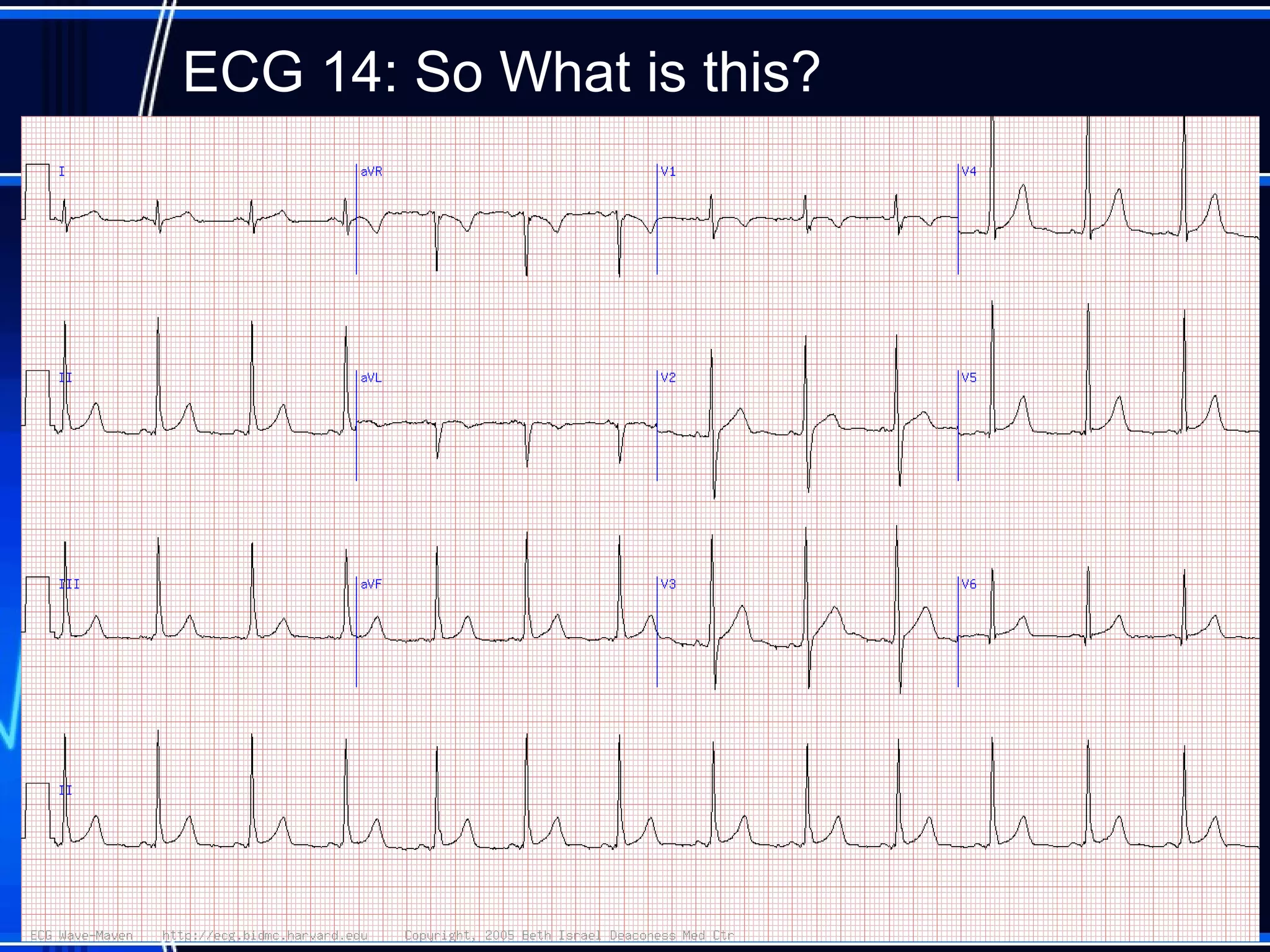


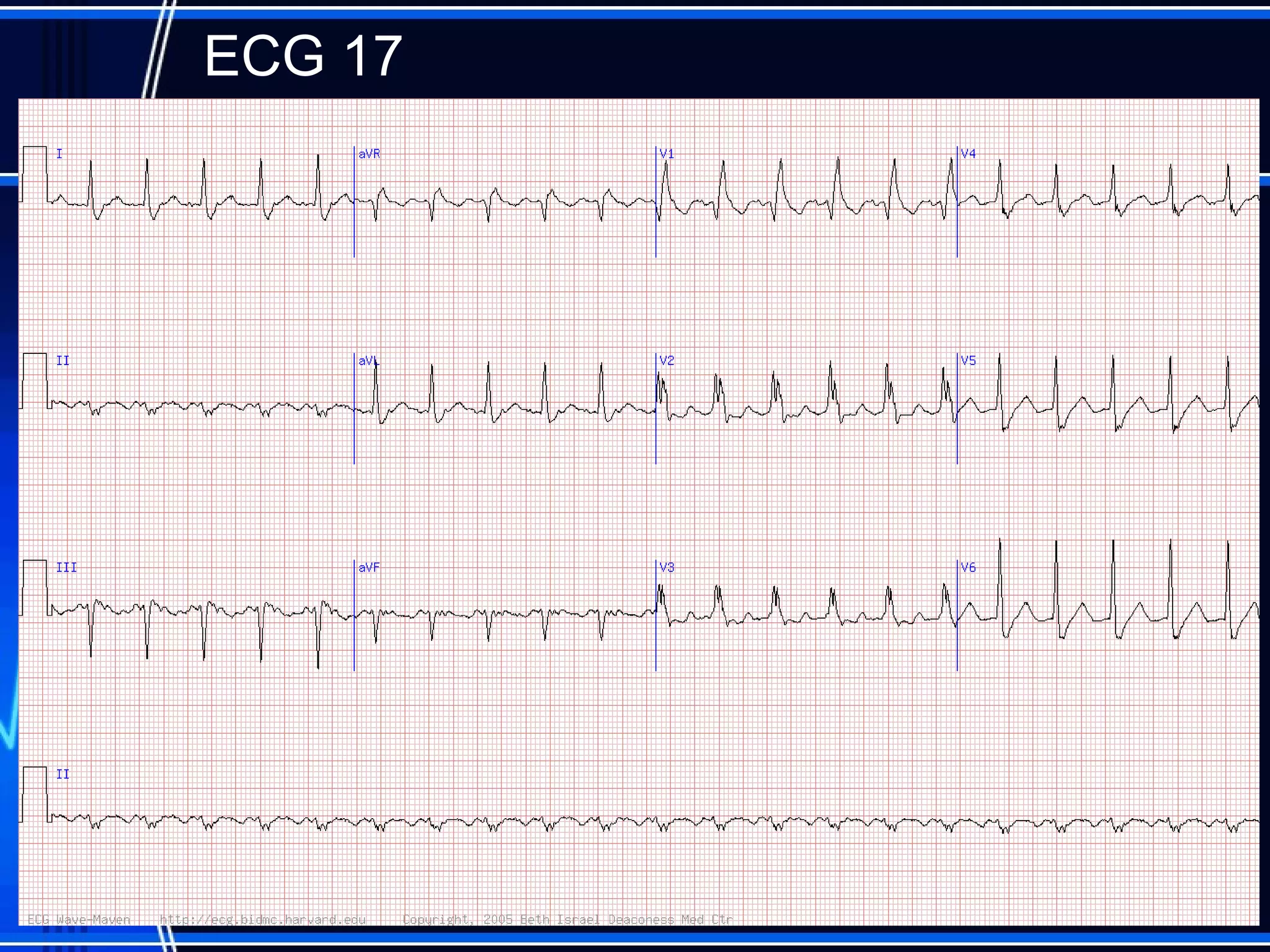

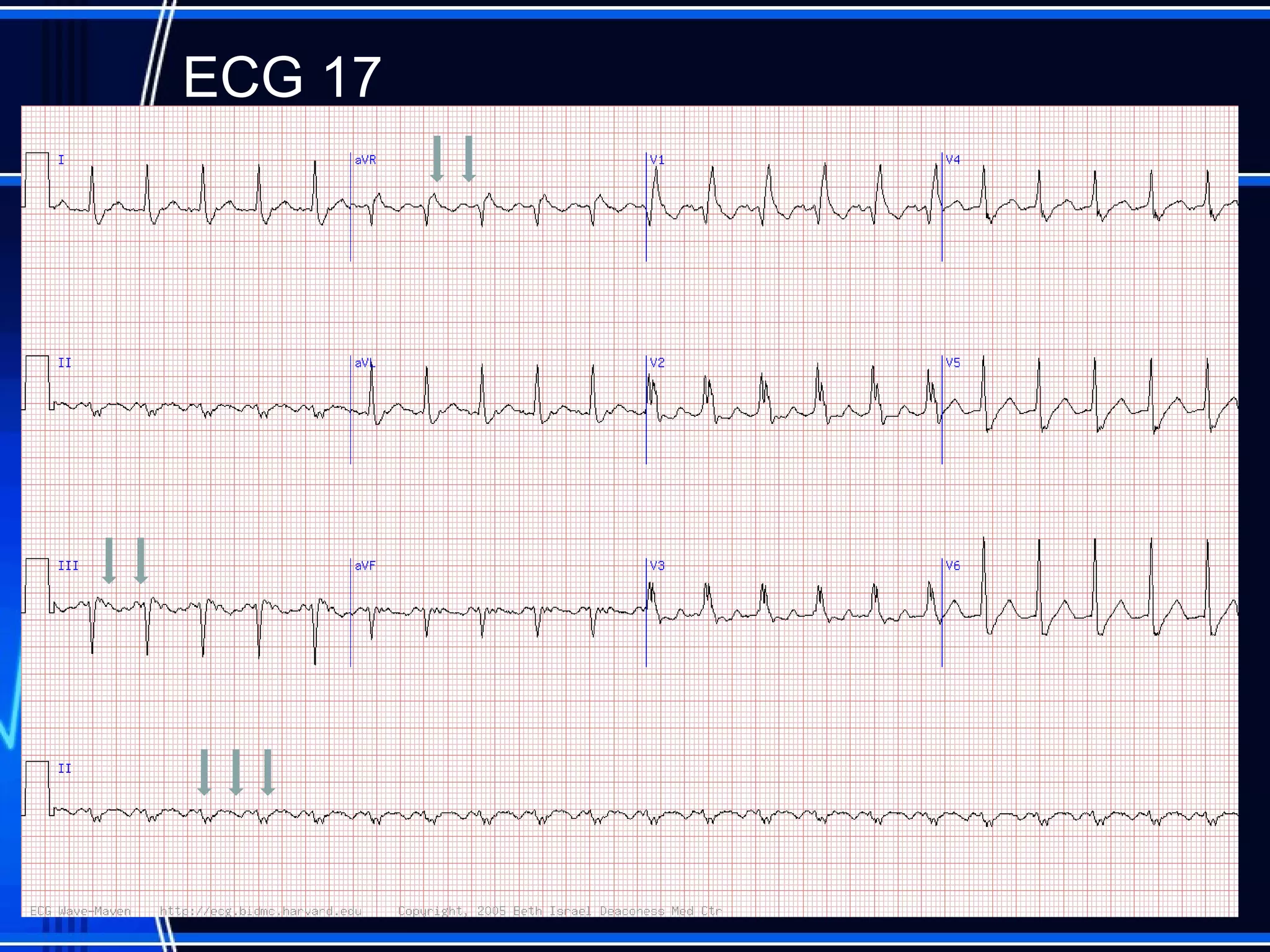

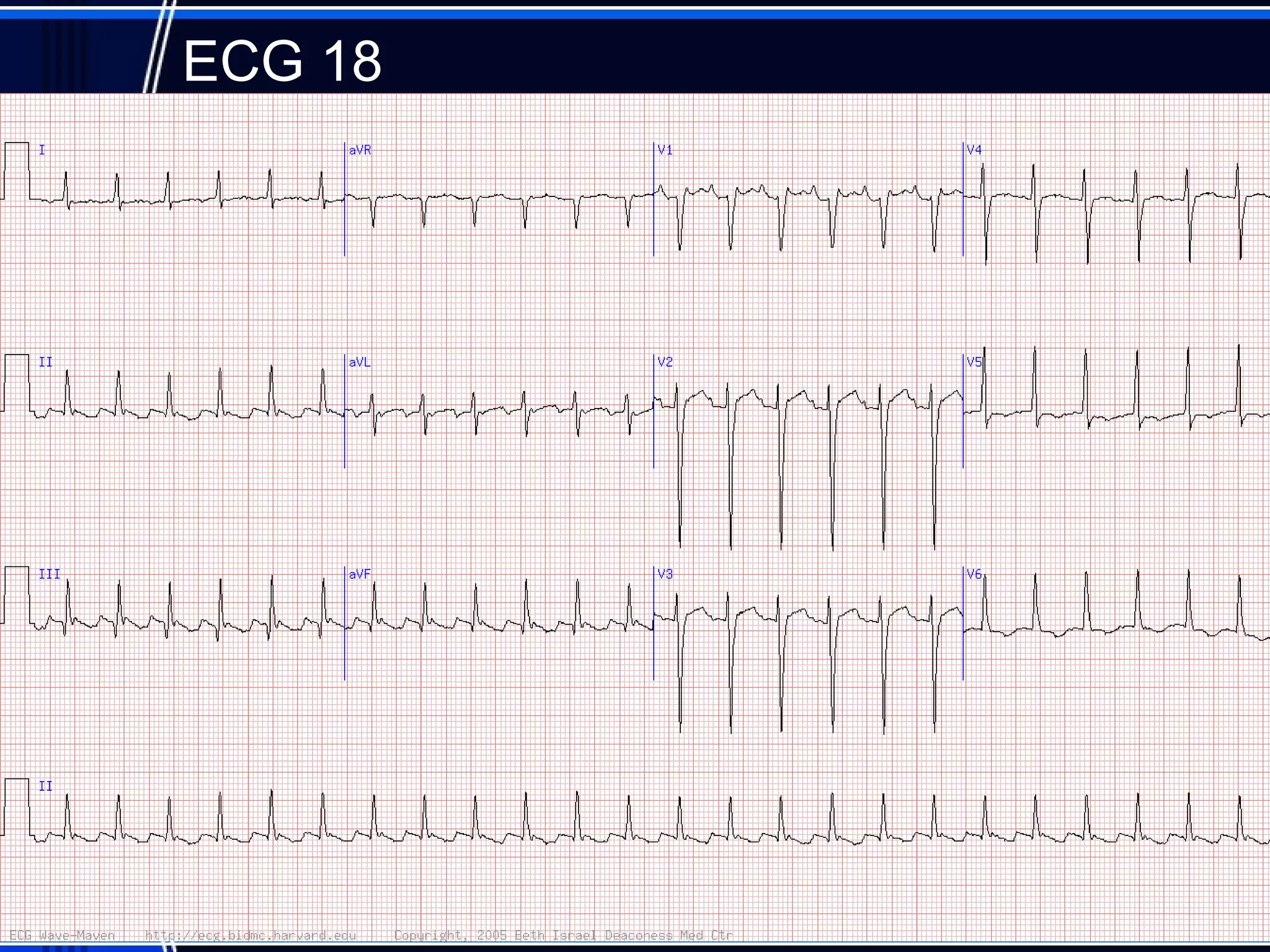
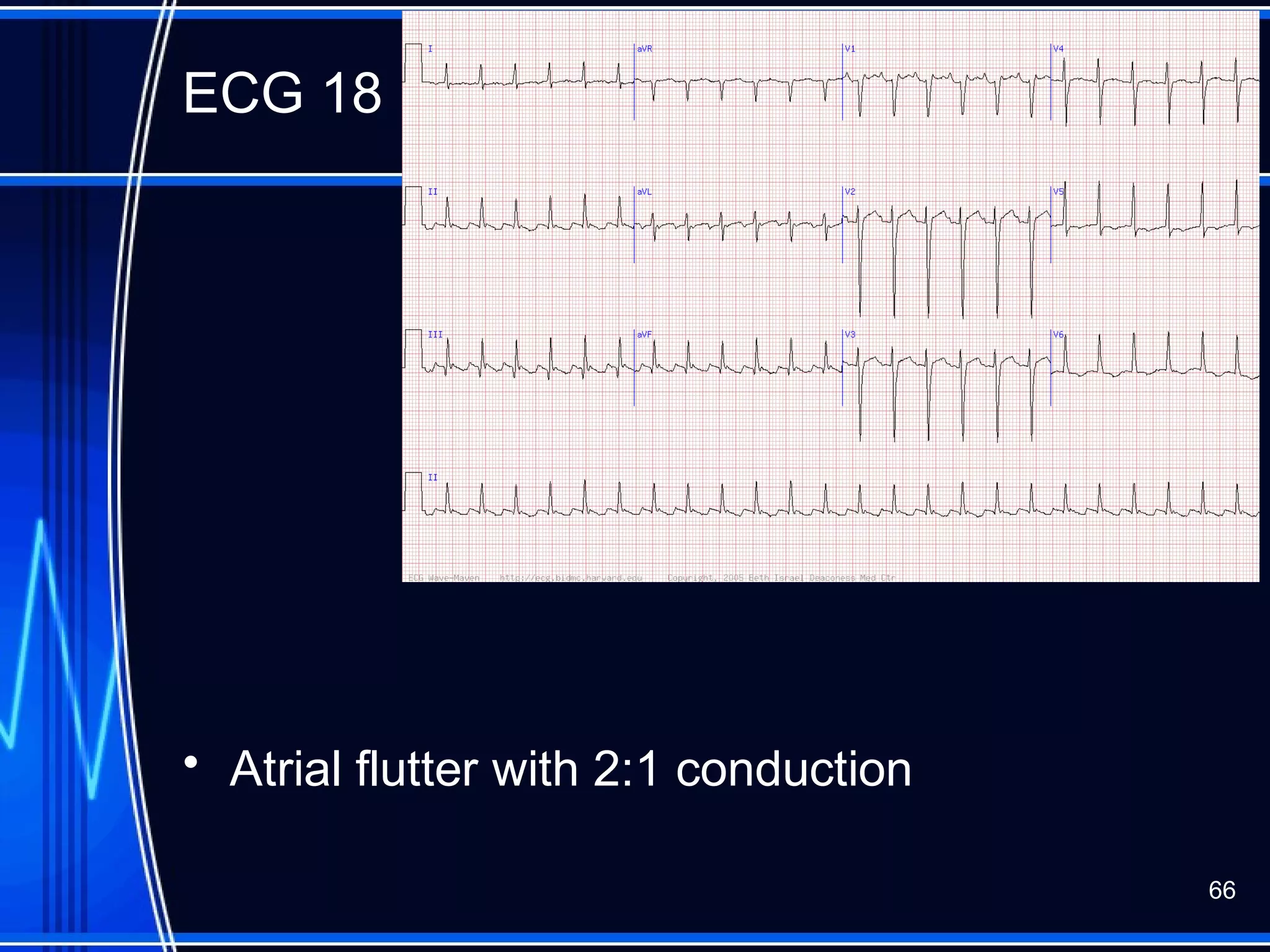

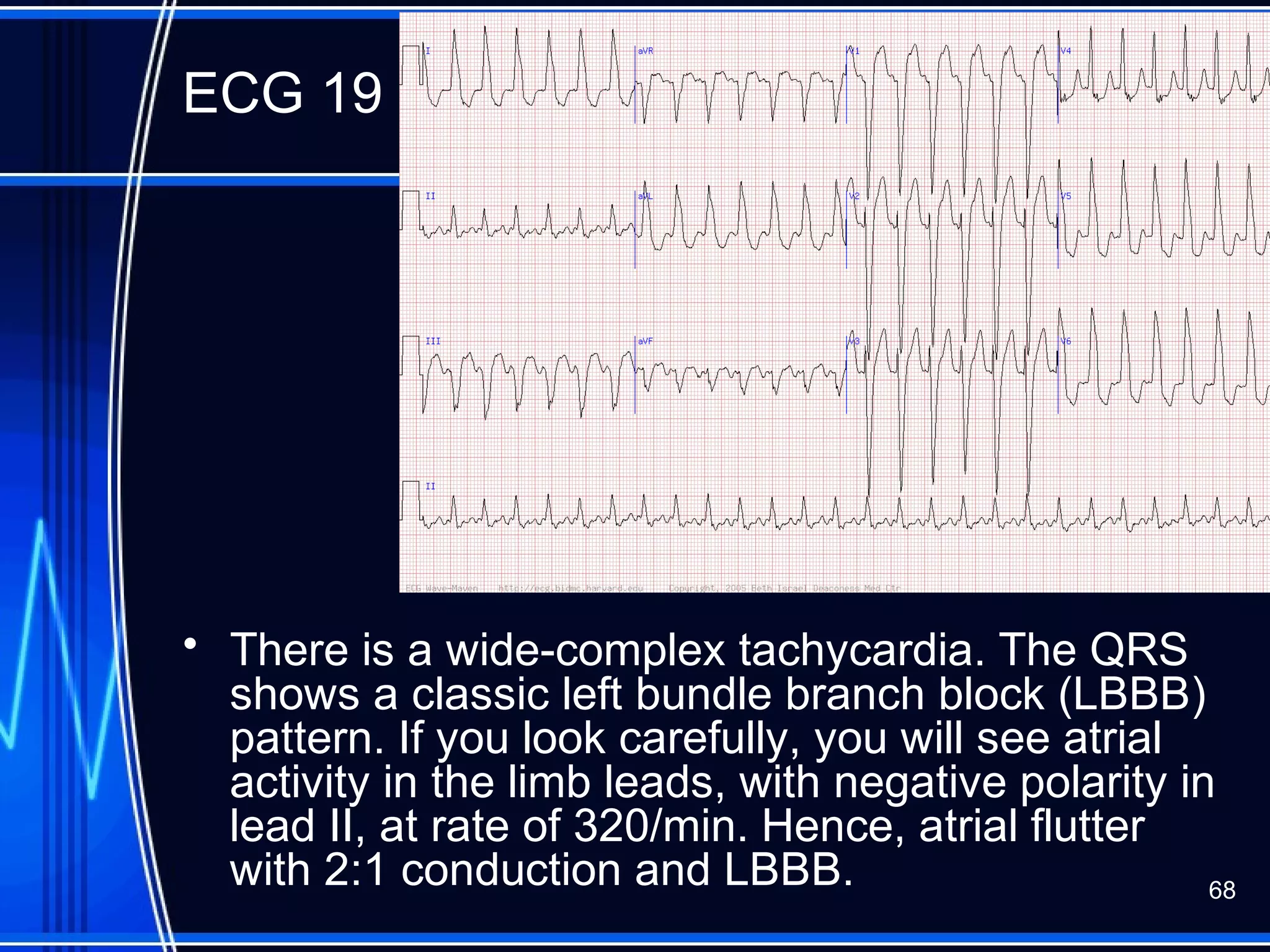



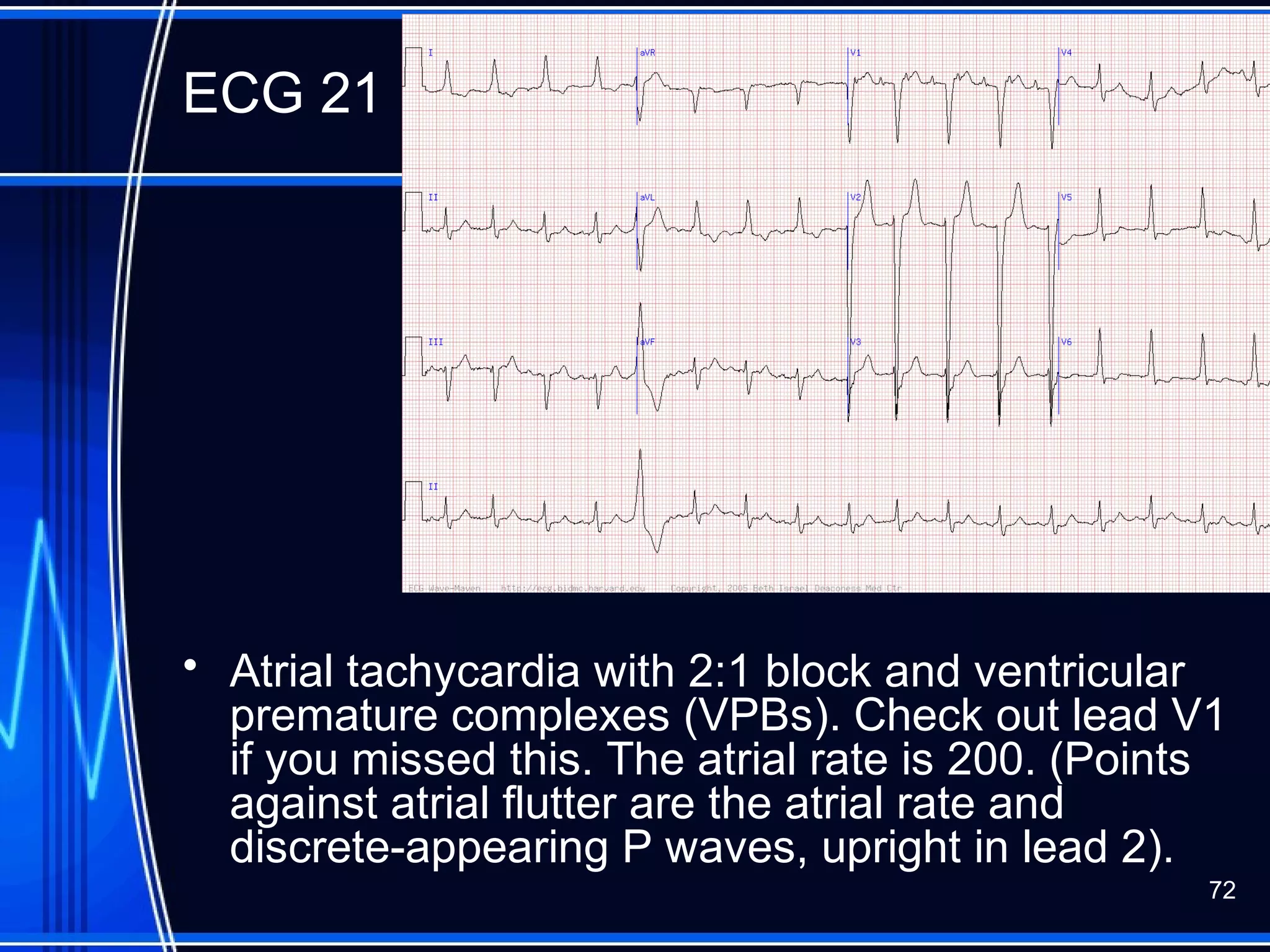
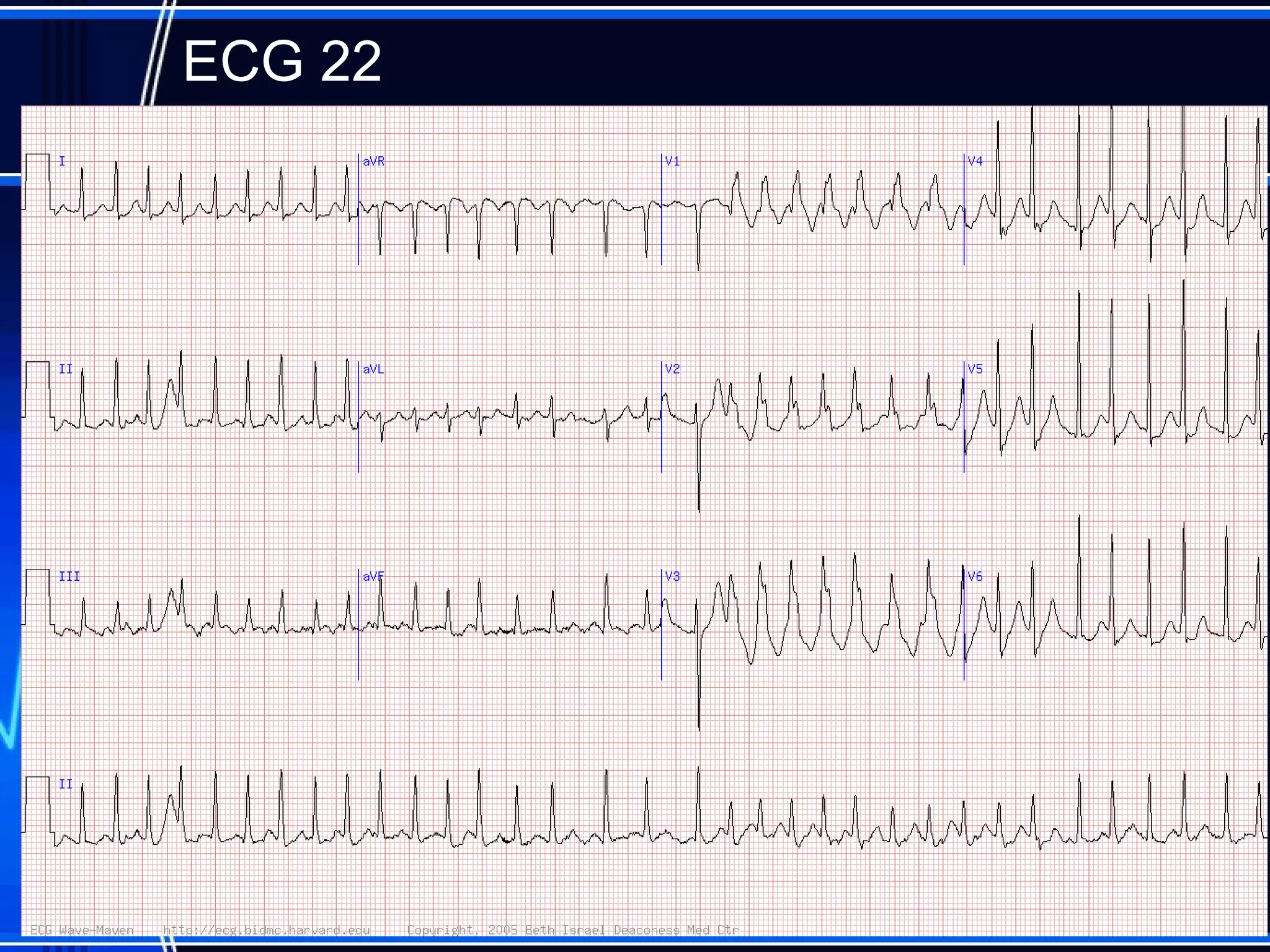













This document provides an overview of approaches to arrhythmias from an electrophysiological perspective. It begins by classifying bradyarrhythmias and tachyarrhythmias based on location and rate. Common supraventricular arrhythmias like AV nodal reentrant tachycardia, atrial flutter, and atrial fibrillation are described. Ventricular arrhythmias including nonsustained and sustained VT are also covered. The document reviews ECG interpretation and provides examples of various arrhythmias, discussing distinguishing characteristics and treatment approaches. Case examples include sinus bradycardia with heart block, Wenckebach block, junctional escape rhythms, atrial flutter, AVNRT, preexcitation













































![ECG [Compatibility Mode].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/ecgcompatibilitymode-230828072404-d338c45c-thumbnail.jpg?width=640&height=640&fit=bounds)