Downloaded 13 times




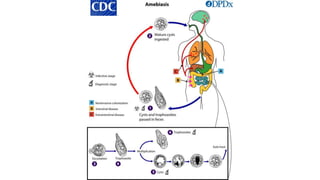

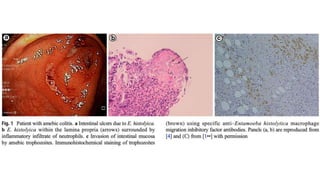
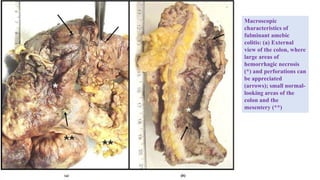
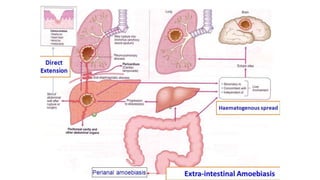
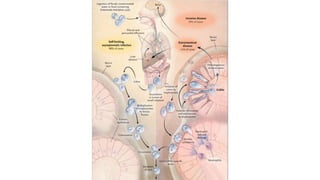











E. histolytica causes a range of diseases in humans. It can cause asymptomatic intestinal infection or symptomatic amebic colitis characterized by diarrhea, abdominal cramps and pain. Rarely, it can cause a severe, fulminant colitis with toxic megacolon. It is also known to cause amebic liver abscess when trophozoites spread from the intestine to the liver via the portal vein. E. histolytica exhibits a complex life cycle alternating between the infective cyst form and the invasive trophozoite form.


















































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)




