Downloaded 27 times















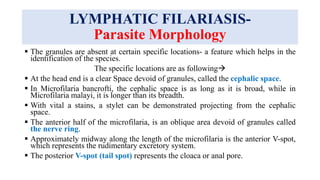





![LYMPHATIC FILARIASIS-
Clinical Manifestations
The most common presentations of lymphatic filariasis are
Symptomatic (subclinical) microfilaremia,
Acute adenolymphangitis (ADL) and
Chronic lymphatic disease.
Most of the patients appear clinically asymptomatic but virtually all of them have
subclinical disease including
Microscopic hematuria or proteinuria,
Dilated lymphatics (visualized by imaging) and in men with W. bancrofti
infection,
Scrotal lymphangiectasia [Lymphangiectases represent superficial lymphatic
dilatation caused by a wide range of scarring processes. Lymphangiectasia occurs
as a consequence of lymphatic damage by an external cause, leading to obstruction
of local lymphatic drainage.] (detected by ultrasound).](https://image.slidesharecdn.com/filarisis-210528105152/85/Filarisis-33-320.jpg)

















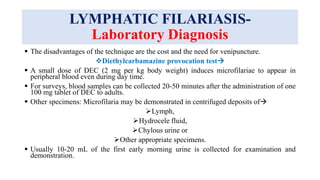










This document discusses lymphatic filariasis, caused by parasitic roundworms transmitted by mosquitoes. It provides details on the life cycle and morphology of the parasites. Clinical manifestations range from asymptomatic microfilaremia to acute adenolymphangitis and chronic manifestations like lymphedema and elephantiasis. Pathogenesis involves blockage of lymph vessels by adult worms and inflammatory responses. Diagnosis is via blood smears to detect microfilariae and treatment aims to eliminate parasites and control symptoms.























































































