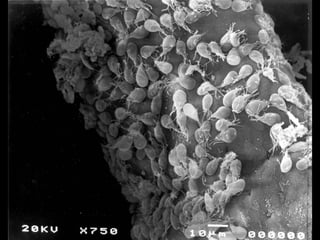
Giardia duodenalis is a flagellated protozoan parasite that causes giardiasis. It has both a trophozoite and cyst stage. The trophozoite lives in the small intestine where it attaches to epithelial cells and feeds on mucus, interfering with absorption. It can cause diarrhea and malabsorption. The cyst forms when trophozoites pass through the large intestine and are excreted in feces. Cysts are hardy and infect new hosts when ingested. Giardiasis is common worldwide and transmitted through contaminated water. Treatment involves metronidazole antibiotics.










































































![3-_Giardia_lamblia[1].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/3-giardialamblia1-230308222541-5f0a9947-thumbnail.jpg?width=640&height=640&fit=bounds)













































