Downloaded 36 times



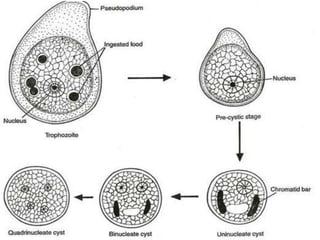





This document provides an overview of Entamoeba, including its classification, morphology, life cycle, virulence factors, transmission, clinical features, diagnosis, and treatment. Key points include: - Entamoeba histolytica is a pathogenic protozoan that can cause intestinal and extra-intestinal infections like amoebic dysentery and liver abscess. - It has three morphological stages - trophozoite, precystic, and cystic stages. Trophozoites cause tissue invasion and disease. - The infective transmissive stage is the mature quadrinucleated cyst which is ingested and excysts in the intestine. - Virulence factors like lect















































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
