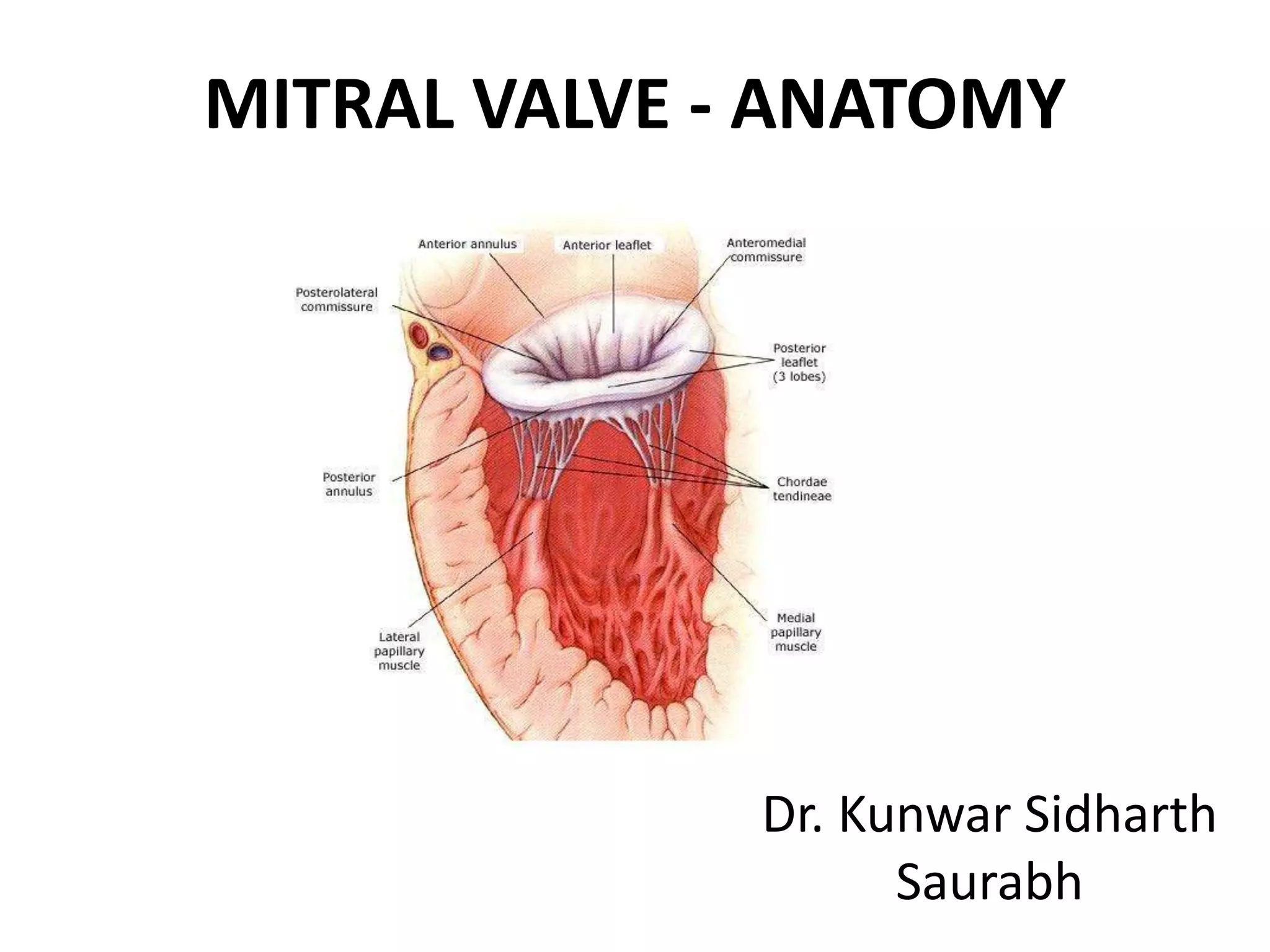
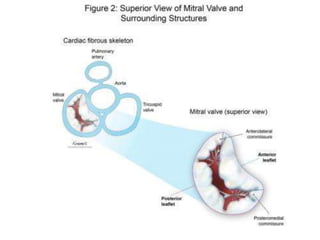
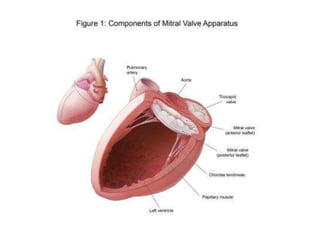
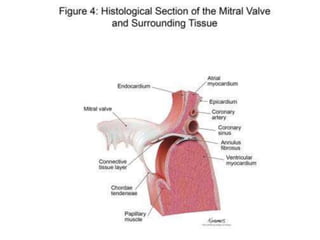
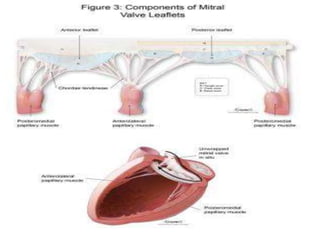
The mitral valve, also known as the bicuspid valve or left atrioventricular valve, lies between the left atrium and left ventricle. It is a dual flap valve made up of the mitral annulus, two leaflets (anterior and posterior), chordae tendineae connecting the leaflets to the papillary muscles of the left ventricle, and the left ventricular wall. The mitral valve apparatus works to ensure unidirectional blood flow from the left atrium to the left ventricle during diastole and prevent backflow during systole.
































![Mitral_Valve_Anatomy_Surgical_Perspective[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/mitralvalveanatomysurgicalperspective1-250701160336-9898ca79-thumbnail.jpg?width=640&height=640&fit=bounds)



























![谷歌留痕技术 [ 𝙩𝙤𝙥 𝟮𝟯𝟯. 𝙘 𝙤𝙢 ]](https://cdn.slidesharecdn.com/ss_thumbnails/top233-260130174328-3833018c-thumbnail.jpg?width=640&height=640&fit=bounds)







