









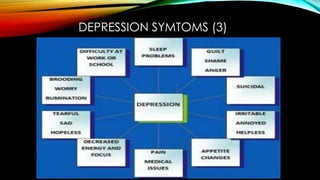




































The document provides an overview of clinical depression, including its symptoms, causes, and treatments. It highlights factors such as chemical imbalances, environmental influences, and deep-seated anger that may contribute to depression, while also discussing various treatment options like psychotherapy, medication, and alternative approaches. Additionally, it emphasizes the importance of support groups and encourages awareness regarding the complexities of depression.











































































































