Downloaded 2,565 times

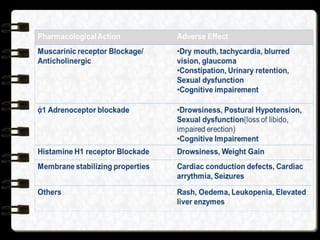
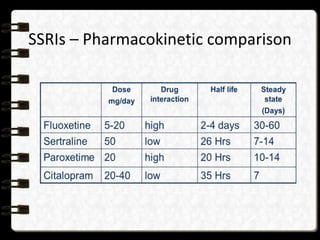
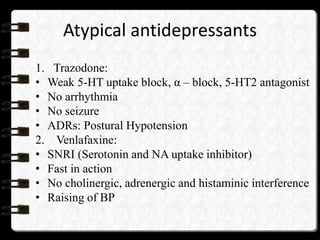
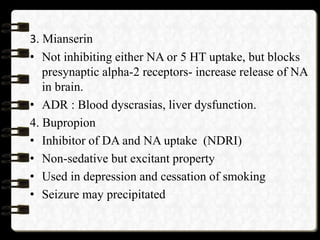
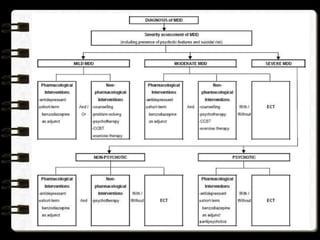
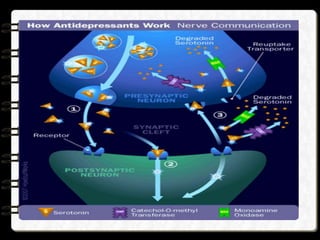


This document provides an overview of depression, including its definition, types, epidemiology, etiology, pathophysiology, clinical manifestations, diagnosis, investigations, and treatment. Depression is defined as a common mental disorder characterized by depressed mood, loss of interest, feelings of guilt, sleep disturbances, low energy, and poor concentration. Major types include major depressive disorder, bipolar disorder, dysthymic disorder, and situational depression. Depression affects over 350 million people globally and is a leading cause of disability. Causes may include genetic, environmental, biochemical and neurological factors. Treatment involves antidepressant medications like SSRIs, TCAs, and MAOIs as well as psychotherapy and other non-pharmacological approaches.



































































































