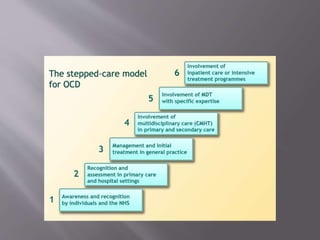
This document provides an overview of obsessive compulsive disorder (OCD), including its definition, symptoms, causes, diagnosis and treatment. OCD is characterized by intrusive thoughts (obsessions) and repetitive behaviors (compulsions) performed to reduce associated anxiety. It has been linked to imbalances in serotonin and dopamine levels in the brain. Treatment involves cognitive behavioral therapy and medication, primarily selective serotonin reuptake inhibitors. The goals of treatment are to reduce symptoms and restore optimal functioning.