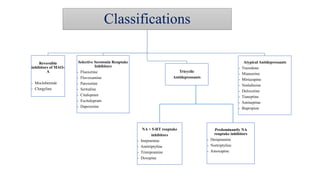
Major depression is a mood disorder characterized by depressed mood or loss of interest in activities. It is estimated that over 300 million people worldwide suffer from depression. Treatment involves psychotherapy such as cognitive behavioral therapy and antidepressant medication. There are several classes of antidepressants including selective serotonin reuptake inhibitors (SSRIs), tricyclic antidepressants, and atypical antidepressants. SSRIs are now the first-line treatment due to their favorable side effect profile compared to other antidepressants. Research is also being conducted to develop new antidepressant drugs with novel mechanisms of action.