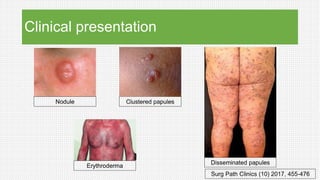
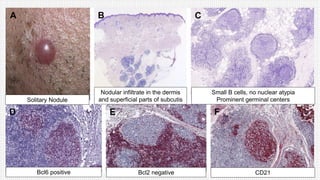
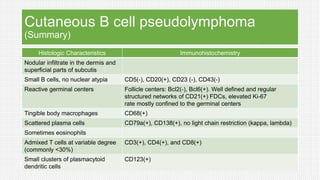
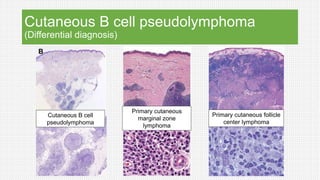
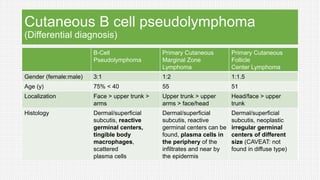
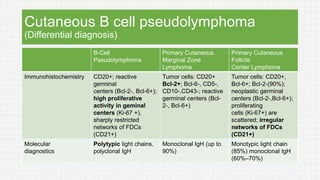
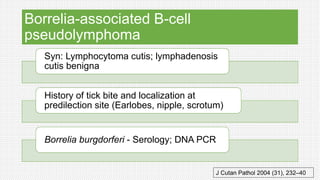
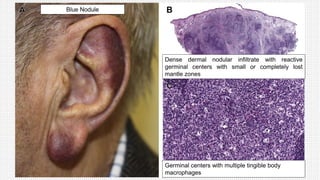
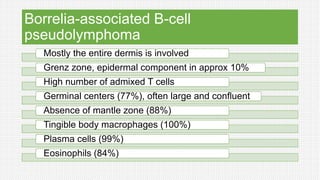
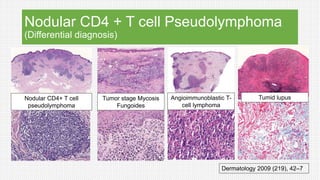
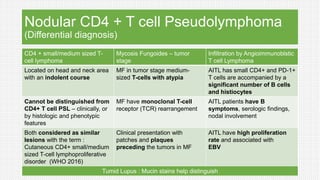
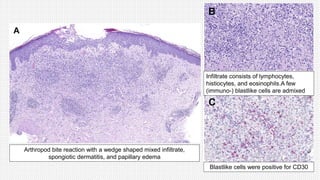
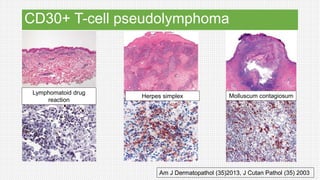
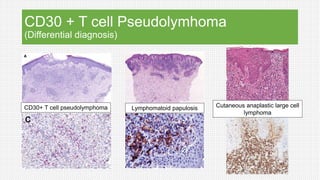
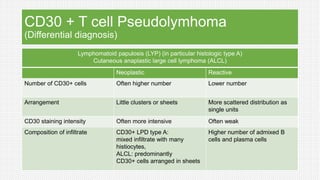
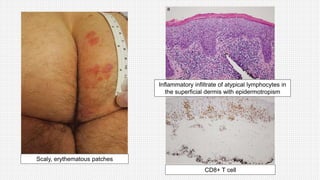
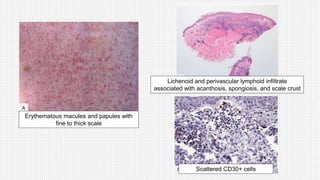
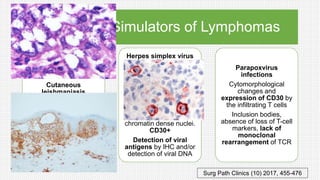
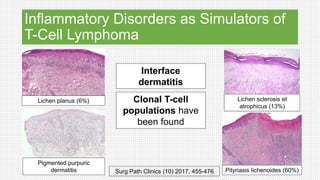
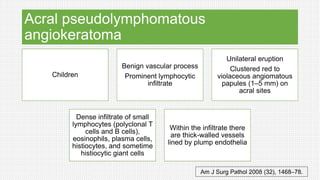
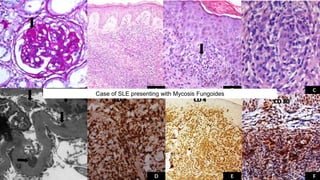
The document discusses cutaneous pseudolymphoma, defining it as a group of skin lesions with lymphocyte-rich infiltrates that mimic cutaneous lymphoma. It provides detailed classifications, clinical presentations, and histopathological features associated with various subtypes, including both T-cell and B-cell pseudolymphomas, their differential diagnoses, and important immunohistochemical markers. Highlights include clinical correlations, important causes, and specific diagnostic considerations for differentiating pseudolymphomas from true lymphomas.











































![GRANULOMATOUS LESION OF SKIN2[299] - Read-Only (1).pptx](https://cdn.slidesharecdn.com/ss_thumbnails/granulomatouslesionofskin2299-read-only1-240725163335-974d6cd5-thumbnail.jpg?width=640&height=640&fit=bounds)











































