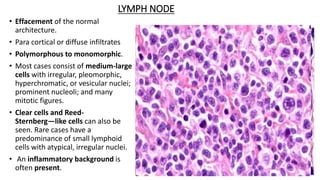
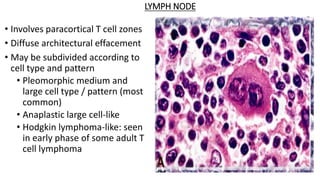
This document provides an overview of T-cell lymphomas, detailing their classification, clinical features, and pathophysiology. It highlights various types, including precursor T-cell neoplasms and mature T-cell neoplasms, along with diagnostic criteria and immunophenotyping characteristics. The document emphasizes the aggressive nature of these malignancies and their association with viral infections, particularly in specific populations.







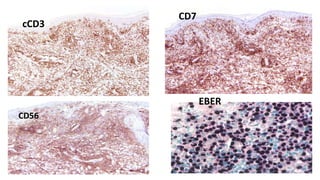


![IMMUNOHISTOCHEMISTRY
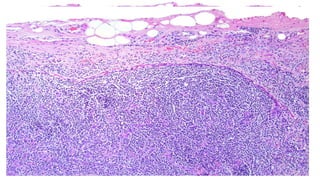
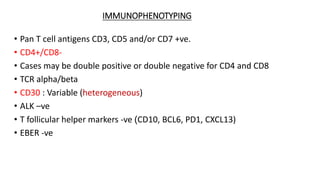
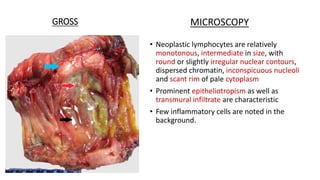
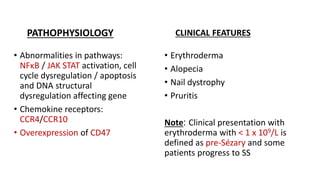
• Diagnosis of exclusion
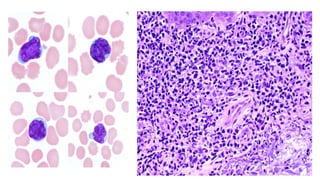
• Mature T cell phenotype ( CD45RO+, TCRβ+, CD2+, CD3+, CD4+
[frequent], CD5+, CD7+) is most commonly observed
• Loss of CD2 or CD5 favors mycosis fungoides
• Partial loss of CD7 is common.
• TCR gamma, CD8 & EBER are negative.](https://image.slidesharecdn.com/tcelllymphomas-230203143134-39451bd9/85/T-cell-lymphomas-By-Dr-MULUKALA-SWETHA-86-320.jpg)





















































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)












![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


