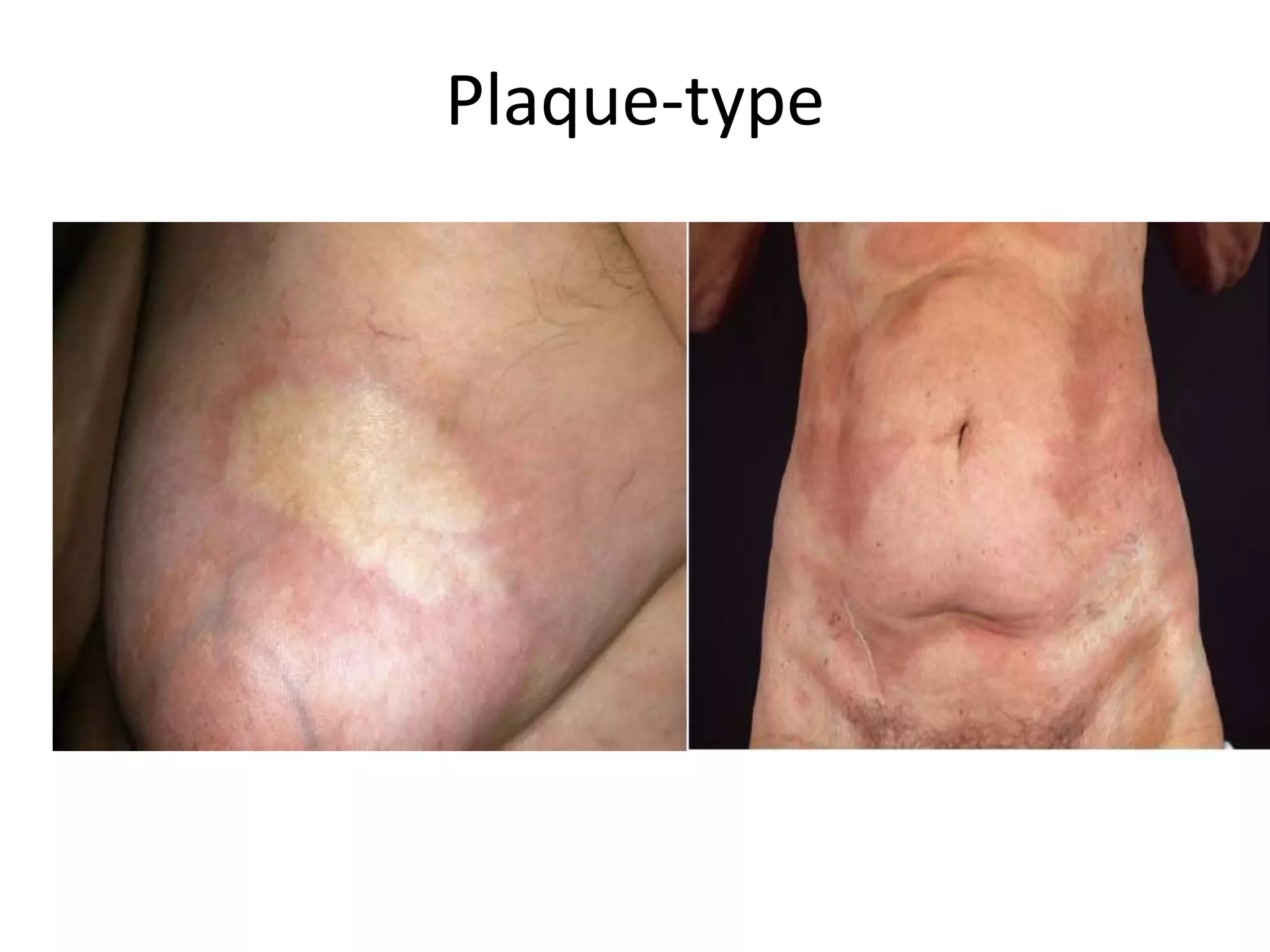
Localized scleroderma (LS), also called morphea, is a rare autoimmune disease that primarily affects the skin, causing hardening and fibrosis. It comes in several subtypes depending on the extent, location, and depth of skin involvement. The most common subtypes are plaque morphea, linear morphea, and generalized morphea. Linear morphea is most common in children and can cause serious complications by restricting growth and movement if not properly treated. While LS only affects the skin, it can lead to significant scarring, contractures, and physical disability depending on the specific subtype and location of lesions.