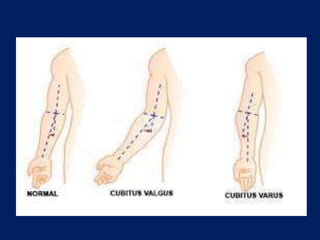
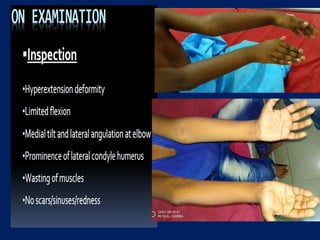
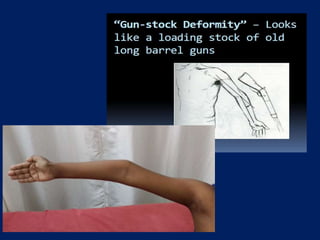
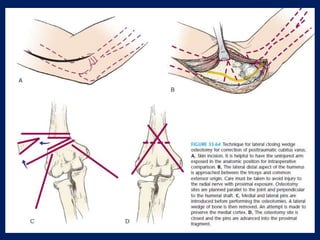
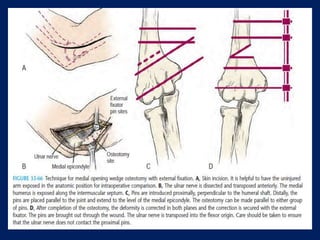
Cubitus varus, or gunstock deformity, is caused by malunion of supracondylar fractures and results in the forearm being deviated inward at the elbow with loss of the carrying angle. It is a triplanar deformity involving varus, hyperextension, and internal rotation. Treatment options include observation for young children, hemiepiphysiodesis to alter growth, and corrective osteotomy. The lateral closing wedge osteotomy is commonly used to safely correct the varus deformity through removal of a lateral wedge. Other techniques include medial opening wedge, oblique, dome, and step-cut osteotomies. Postoperative management focuses on immobilizing the arm in extension