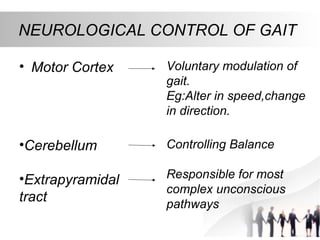
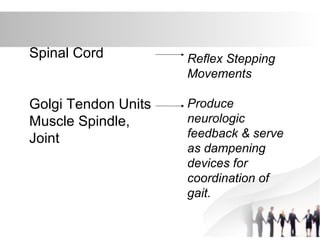
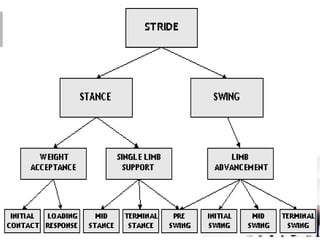
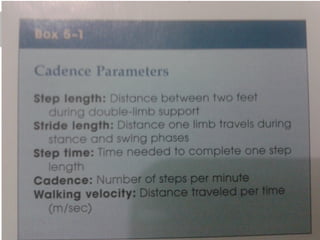
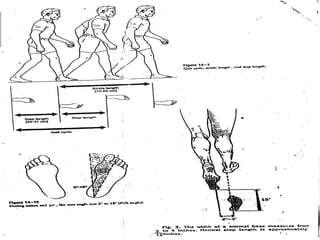
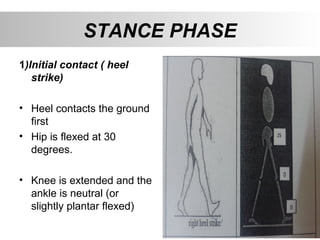
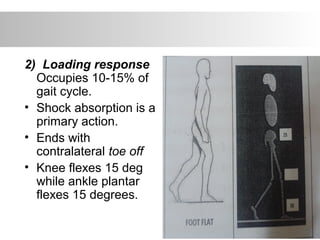
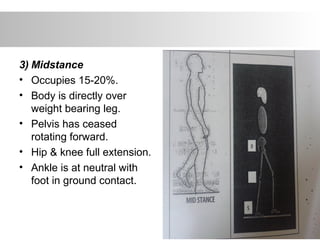
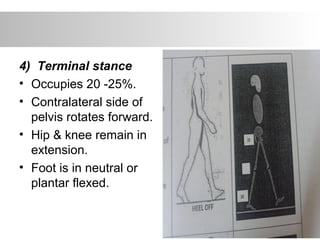
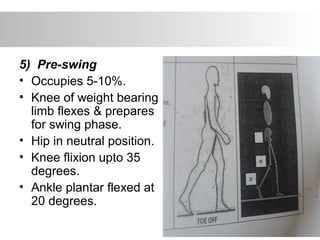
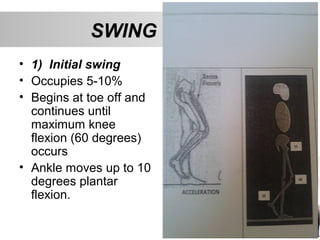
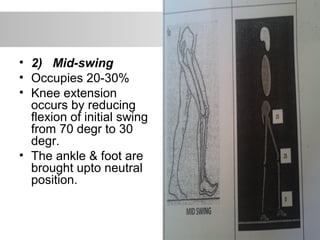
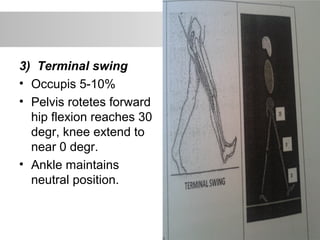
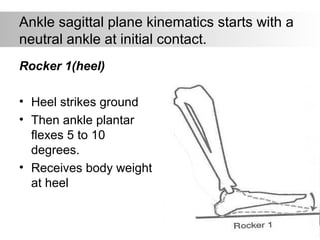
This document summarizes gait cycle and pathological gait. It describes the normal gait cycle which consists of stance and swing phases. Stance phase is about 60% of the cycle and is divided into initial contact, loading response, midstance, terminal stance, and pre-swing. Swing phase is 40% and includes initial swing, midswing, and terminal swing. Neurological control, kinematics, determinants, muscle activity, and kinetics of normal gait are also outlined. Pathological gait due to various causes like muscle weakness, deformities, and neurological disorders are discussed. Benefits of gait analysis for diagnosis and treatment are provided in the conclusion.






































![GAIT and its different types[Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/gaitautosaved-240815185755-7939fafe-thumbnail.jpg?width=640&height=640&fit=bounds)
















































