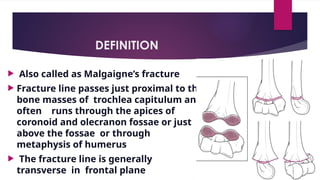
DEFINITION
Also calledas Malgaigne’s fracture
Fracture line passes just proximal to the
bone masses of trochlea capitulum and
often runs through the apices of
coronoid and olecranon fossae or just
above the fossae or through
metaphysis of humerus
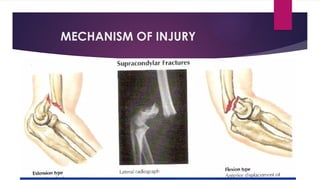
The fracture line is generally
transverse in frontal plane
Remodeling ofbone causes decreased AP diameter in the
SUPRACONDYLAR region, making this area susceptible to injury
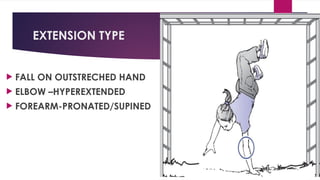
Ligamentous laxity increases the likelihood of hyper extension injury
Anterior capsule is thicker and stronger than posterior capsule. In
extension,the fibers of anterior capsule is taut, serving as fulcrum by
which olecranon becomes firmly engaged in olecranon fossa. With
extreme force ,hyperextension may cause olecranon process to
impinge on superior olecranon fossa and SUPRACONDYLAR region
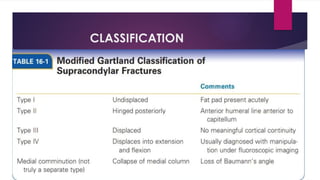
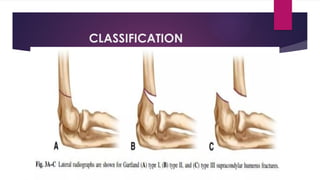
TYPE II
Displaced#>2mm
AHL goes anterior to
capitulum
Posterior cortical
contact intact
13.
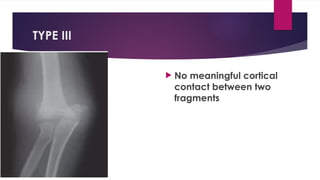
TYPE III
Nomeaningful cortical
contact between two
fragments
14.
TYPE IV
Multidirectionalinstability
Diagnosed
intraoperatively In
extension capitulum lies
posterior to AHL & In
flexion capitulum lies
anterior to AHL
15.
CLINICAL EVALUATION
Inmost cases, children children will not move
the elbow if a fracture is present, although
this may not be the case for non-displaced
fractures.although this may not be the case
for non-displaced fractures.
Swelling about elbow is a constant feature,
develop within first few hrs.
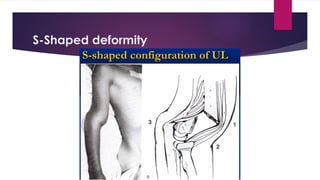
S shaped deformity
Distal humeral tenderness
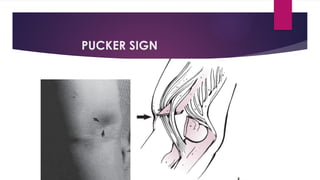
Anterior plucker sign +ve
BAUMANN’S ANGLE
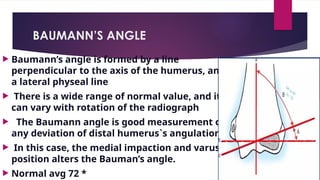
Baumann’sangle is formed by a line
perpendicular to the axis of the humerus, and
a lateral physeal line
There is a wide range of normal value, and it
can vary with rotation of the radiograph
The Baumann angle is good measurement of
any deviation of distal humerus`s angulation
In this case, the medial impaction and varus
position alters the Bauman’s angle.
Normal avg 72 *
21.
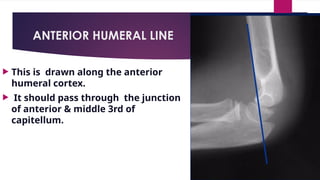
ANTERIOR HUMERAL LINE
This is drawn along the anterior
humeral cortex.
It should pass through the junction
of anterior & middle 3rd of
capitellum.
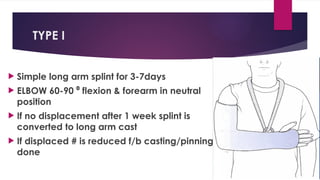
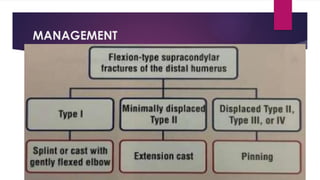
TYPE I
Simplelong arm splint for 3-7days
ELBOW 60-90 flexion & forearm in neutral
⁰
position
If no displacement after 1 week splint is
converted to long arm cast
If displaced # is reduced f/b casting/pinning
done
25.
TYPE II
CMRF/B SELECTIVE PINNING WITH SUPPOTIVE
LONG ARM SPLINT
26.
TYOE III ANDIV
Unstable
Periosteum is torn
No cortical contact between two fragments
Associated with soft tissue injury
Reduction (closed/open)
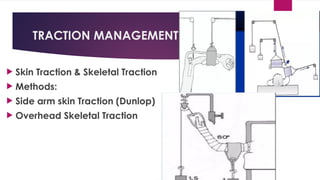
Stabilisation (PINS/TRACTION MANAGEMENT)
27.
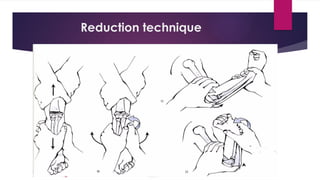
Reduction technique
Tractionand counter traction
Milking maneuver
Correction of medial/lateral displacement
Correction of rotational deformities
Correction of posterior displacement by flexion maneuver
ELBOW held in hyper flexion
Forearm held in pronation/supination
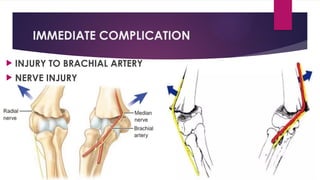
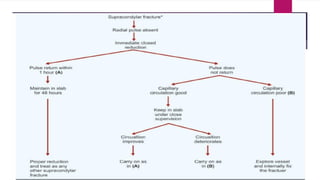
COMPLICATION
IMMEDIATE COMPLICATION:at the time of
Fracture
EARLY COMPLICATION:within first 2-3days
LATE COMPLICATION:Weeks to months after
Fracture
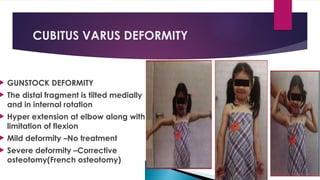
CUBITUS VARUS DEFORMITY
GUNSTOCK DEFORMITY
The distal fragment is tilted medially
and in internal rotation
Hyper extension at elbow along with
limitation of flexion
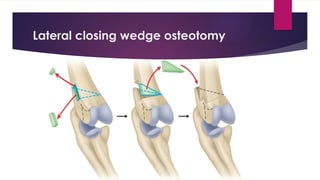
Mild deformity –No treatment
Severe deformity –Corrective
osteotomy(French osteotomy)
































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)



![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)






