Supracondylar osteotomy for treatment of cubitus varus

This meta-analysis reviewed 40 studies on supracondylar osteotomy for treating cubitus varus deformity in children. It found that lateral wedge osteotomy was the most common procedure, achieving 84% excellent results in correcting the deformity and restoring carrying angle. On average, procedures corrected 27 degrees of varus deformity and improved range of motion by 20 degrees. Major complications occurred in less than 10% of cases and included residual deformity, nerve injury, infection, and loss of fixation. The study found equivalent results across treatment methods but noted k-wire fixation had a higher risk of complications compared to screws or external fixation. It recommends surgeons choose treatment based on individual case factors and discuss risks and expectations thoroughly with parents.

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to Supracondylar osteotomy for treatment of cubitus varus
Similar to Supracondylar osteotomy for treatment of cubitus varus (20)
Recently uploaded
Recently uploaded (20)
Supracondylar osteotomy for treatment of cubitus varus
- 1. Supracondylar osteotomy for treatment of cubitus varus in children A systematic review published in The bone and Joint Journal, May 2014 Presented by : Harjot Singh Gurudatta Moderator : DR. GAGAN KHANNA
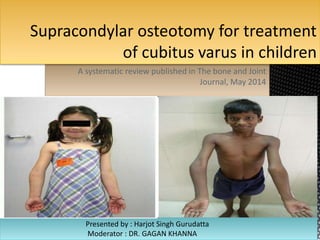
- 2. INTRODUCTION Cubitus varus is the most common significant late complication of supracondylar fracture. This deformity typically represents fracture malunion and rarely results from partial growth arrest of the medial condylar growth plate. Malunion may be avoided by careful attention to anatomic reduction and secure fixation at the time of initial management. Cubitus varus is generally considered a cosmetically acceptable deformity, but increased risk of lateral condyle fracture, tardy ulnar palsy, posterolateral rotary instability of the elbow, and posterior shoulder instability has also been reported. Also, increased awareness among parents has resulted in more children seeking attention
- 3. WHY OPERATE? An increased risk of fracture,especially of the lateral condyle, has been linked with cubitus varus deformity. tardy posterolateral rotatory instability Less flexion and hyperextention Tardy ulnar nerve palsy also has been associated with cubitus varus and internal rotational malalignment. With a cubitus varus deformity, the olecranon fossa moves to the ulnar side of the distal humerus, and the triceps shifts a bit ulnarward. Investigators theorized that this ulnar shift might compress the ulnar nerve against the medial epicondyle, narrowing the cubital tunnel and resulting in chronic neuropathy. Also, a fibrous band running between the heads of the flexor carpi ulnaris was thought to cause ulnar nerve compression.
- 4. TREATMENT OPTIONS Medial displacement and rotation of the distal fragment have been cited most often, but experimental studies showed that varus tilting of the distal fragment was the most important cause of change in the carrying angle. Other suggested causes include varus tilting of the distal fragment and growth disturbance in the distal humerus, especially overgrowth of the lateral condyle. Osteonecrosis and delayed growth of the trochlea, with relative overgrowth of the normal lateral side of the distal humeral epiphysis, is a rare cause of progressive cubitus varus deformity after supracondylar fracture. Accordingly, We can either go for (i) observation with expected remodeling, (ii) hemiepiphysiodesis and growth alteration, and (iii) corrective osteotomy. Observation is not recommened in this era. Hemiepiphysiodesis is also seldom recommended as the distal humerus accounts for only 20% of Humeral growth and even less in the >6yrs age group. Three basic types of osteotomies have been described: a medial opening wedge osteotomy with a bone graft, an oblique osteotomy with derotation, and a lateral closing wedge osteotomy. The latter being the most popular.
- 8. This study is a metaanalysis of various studies conducted for cubitus varus deformity correction. A total of 330 studies were shortlisted out of which 40 were selected for this analysis based on no. of cases, age, operative technique and many other factors. Outcome assessment was done according to the correction achieved, ROM attained,alignment ,complications, function etc. Major complications included Residual deformity, nerve injury, infection, loss of fixation, stiffness. Good correction with <5 deg varus with good function without pain and no complications were included as excellent result
- 9. RESULTS Lateral wedge osteotomy was the main method of treatment in 24 of the studies, with 473 patients resulting in 84% excellent results Distraction osteogenesis was done in 2 studies, 37 patients with equivalent results. Dome and complex(multiplanar) osteotomy done in 7 studies, 100 patients with 90% excellent results. The most common fixation method used were k wires(46%), ex-fix(12%), Tension band with screws(11%), screw(8%), plates(4%). Mean preop carrying angle was 20 deg varus and postop 7 deg valgus, with around 27 deg correction. Mean time to union was 8 weeks, and mean ROM improved by 20 deg. Nerve injury incidences and infection were uncommon mean being 2 % in all groups. Most common complication was residual varus , Being 6% in all groups As far as fixation method is concerned , 20% of those with k – wires sustained complications(infection(3%), residual varus(10%), loss of fixation). Screws alone and Ex-fix had the lowest complications., But the p value was insignificant.
- 10. Approach also had no differnce in complications with 2% nerve injuries in all post med or lat approach This study found the results to be similar in all study groups in terms of complications, and effectiveness. This study recommends the surgeons to chose the method of treatment with care and as per the norms in their locality, practice and teaching. It is most important to take the parents in confidence with detailed discussions regarding the possible complications, fixation method, functional outcome and residual deformity