This document discusses brachial plexus injuries, including:
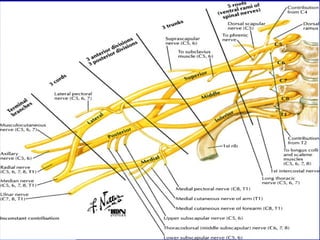
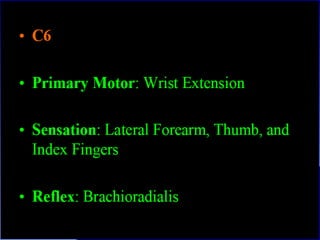
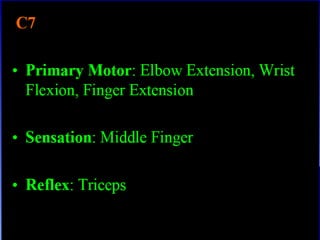
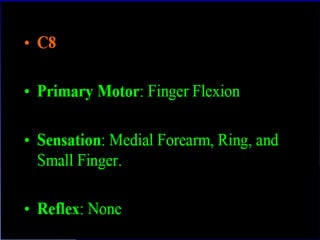
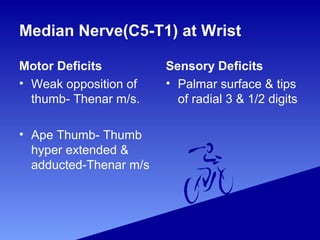
- The brachial plexus is formed from spinal nerve roots C5-T1 and provides motor/sensory function to the shoulder, arm, and hand.
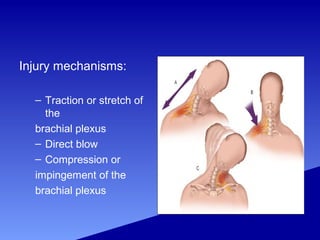
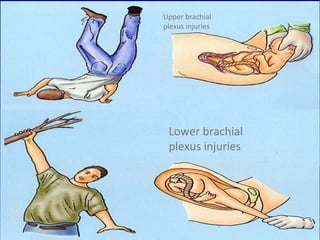
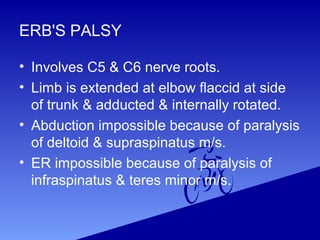
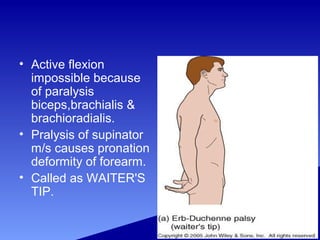
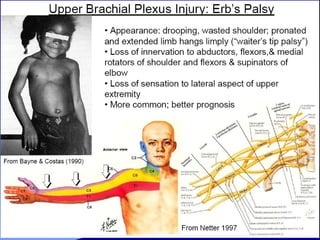
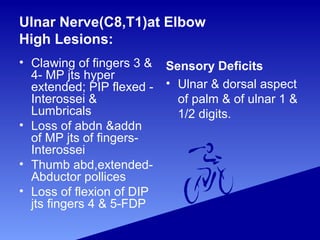
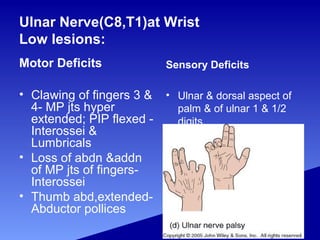
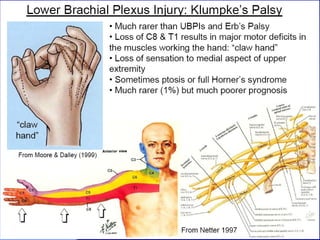
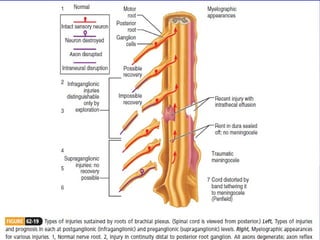
- Injuries can be classified as upper (C5-C6) or lower (C8-T1) plexus injuries and can result from traction, blows, or compression.
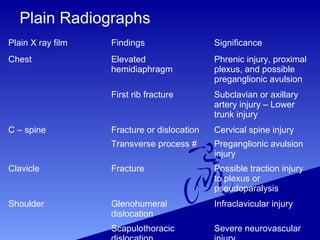
- Evaluation involves imaging, electrodiagnostic tests, and assessing individual nerve deficits.
- Management depends on if the injury is open or closed. Exploration and repair may be done for open injuries, while closed injuries may recover on their own or later require exploration.
-









































![Odu%20 clinical%20science%20iii%20bpi%202011[1]](https://cdn.slidesharecdn.com/ss_thumbnails/odu20clinical20science20iii20bpi2020111-111213214145-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)























































