
Download as PPSX, PPTX

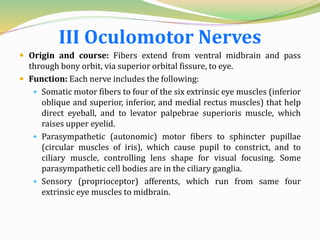
![ Clinical testing: Examine pupils for size, shape, and
equality. Test pupillary reflex with penlight. Test
convergence for near vision and subject's ability to
follow objects with the eyes.
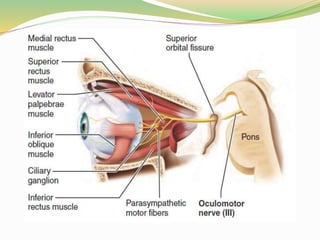
Applied anatomy:- In oculomotor nerve paralysis,
eye cannot be moved up, down, or inward. At rest, eye
rotates laterally [external strabismus] because the
actions of the two extrinsic eye muscles not served by
cranial nerves III are unopposed. Upper eyelid droops
(ptosis), and the person has double vision and trouble
focusing on close objects.](https://image.slidesharecdn.com/cranialnerves-181202085556/85/Cranial-nerves-10-320.jpg)
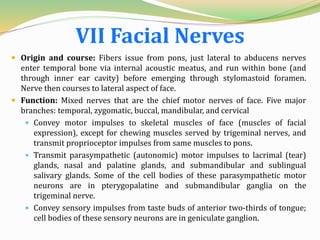
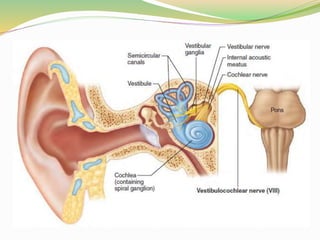
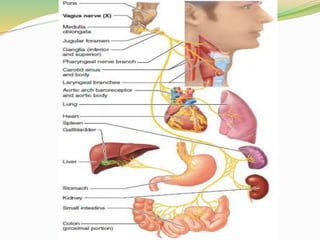
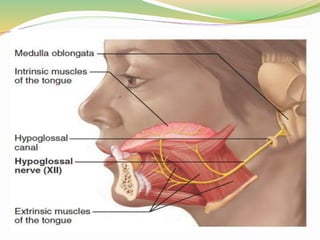
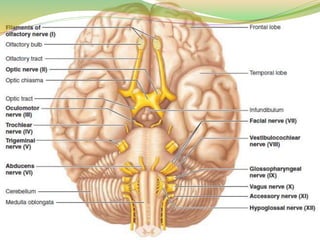
The twelve pairs of cranial nerves serve the brain and structures of the head and neck. The first two pairs attach to the forebrain while the others are associated with the brain stem. Each nerve has a unique origin, course, functions and clinical implications. Damage to specific cranial nerves can impact functions like smell, vision, eye and facial muscle movement, hearing, balance, swallowing, speech and others.
















































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)



![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)


