Downloaded 1,179 times
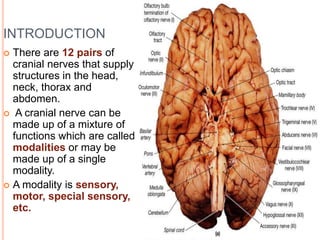
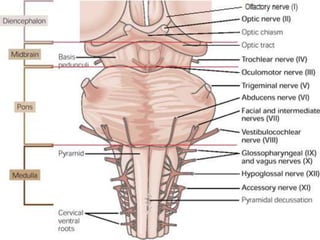
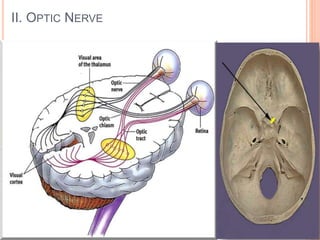
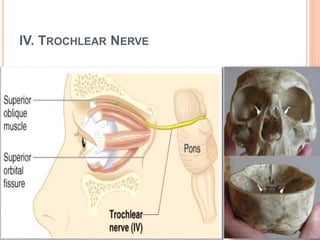
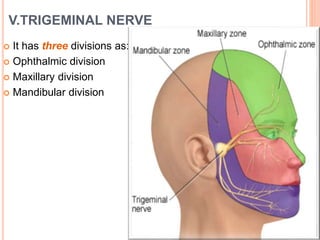
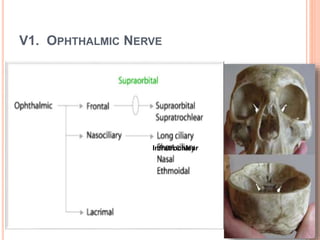
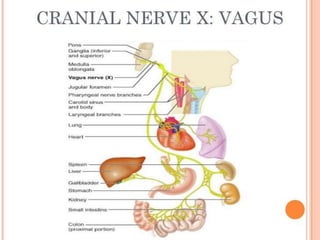
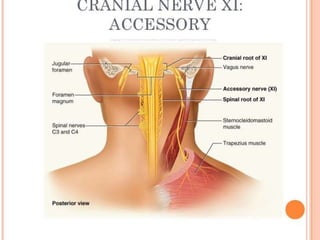


There are 12 pairs of cranial nerves that supply structures in the head, neck, and upper body. They have various functions including sensory, motor, and special sensory roles. The presentation describes each of the 12 cranial nerves - their modality, function, origin, path through the skull, attachments, and clinical effects of damage. The cranial nerves have important roles in vision, smell, hearing, facial muscle control, swallowing, breathing, and other critical functions.























































































