Downloaded 102 times
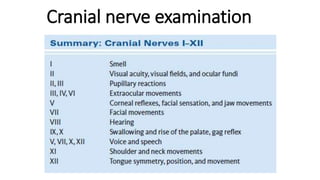
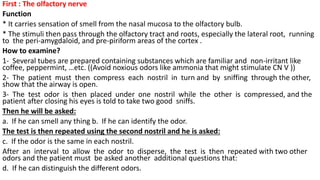
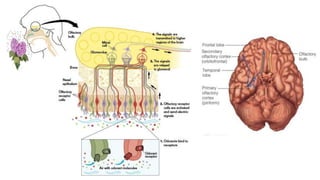
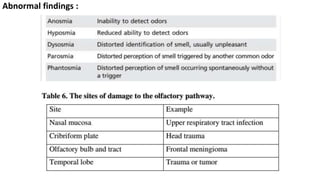
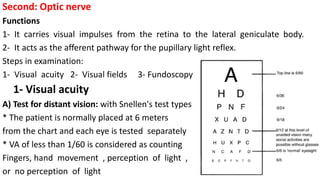
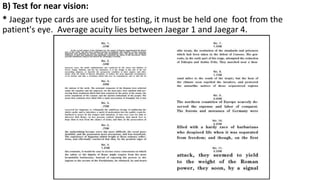
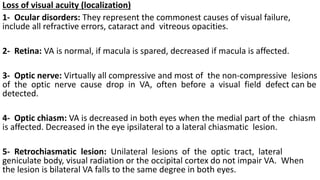
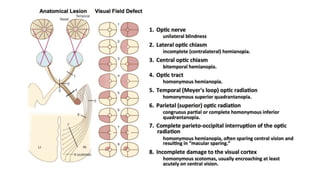
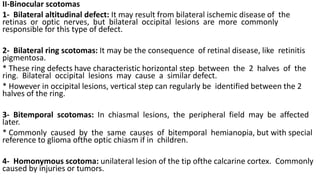
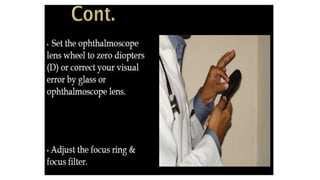
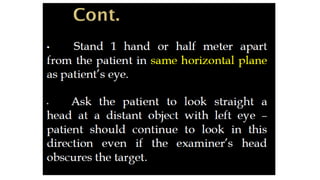
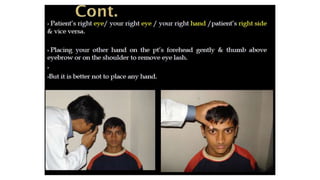
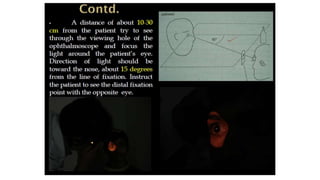




The document summarizes the examination of cranial nerves I (olfactory) and II (optic). For CN I, it describes how to test smell by having the patient identify familiar odors in each nostril. Abnormal findings include inability to smell or distinguish between odors. For CN II, it outlines steps to test visual acuity, visual fields, and fundoscopy. It describes various visual field defects caused by lesions in the eye, optic nerve, chiasm, tract, or occipital cortex and how they present. Features to examine on fundoscopy include color, contour, size, elevation, and neuroretinal rim of the optic disc.
















































































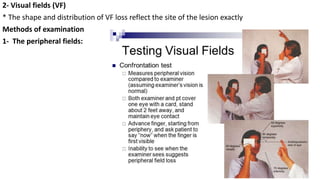
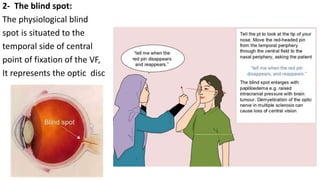
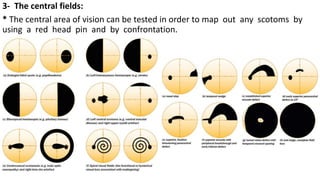
![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)


