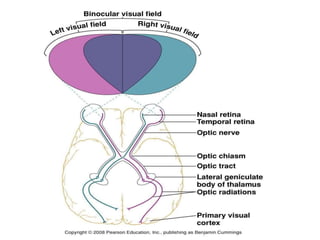
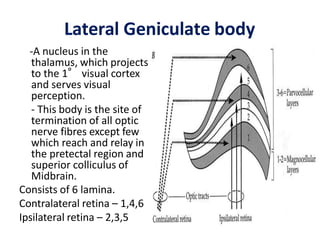
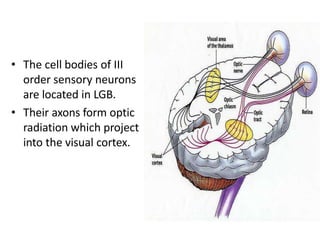
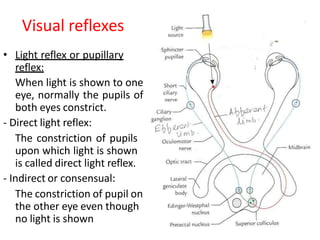
1) The visual pathway consists of the optic nerve, optic chiasm, optic tract, lateral geniculate body, optic radiations, and visual cortex.
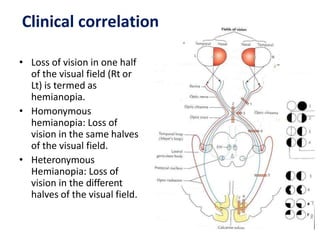
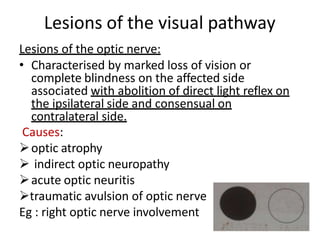
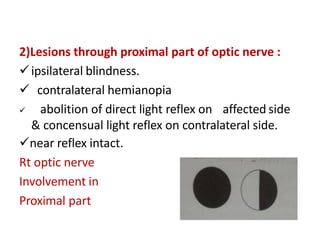
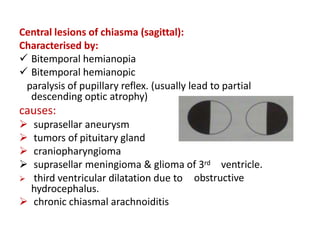
2) Lesions in different parts of the visual pathway cause different visual field defects. For example, a lesion of the optic nerve results in blindness on the affected side while a lesion of the optic chiasm causes bitemporal hemianopia.
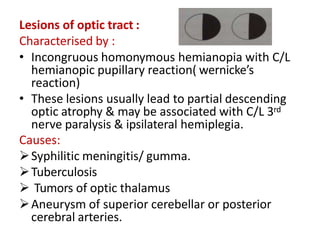
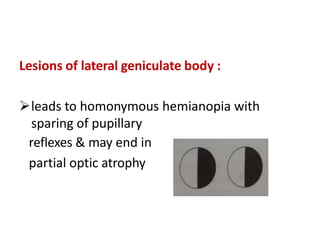
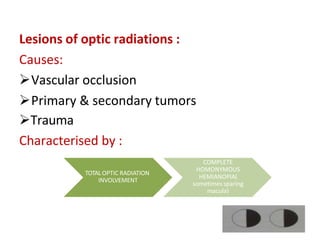
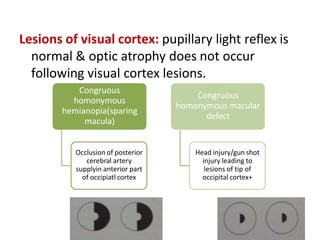
3) Other visual field defects include homonymous hemianopia from lesions of the optic tract, lateral geniculate body, or optic radiations. Lesions of the parietal or temporal lobes can cause quadrantanopia.