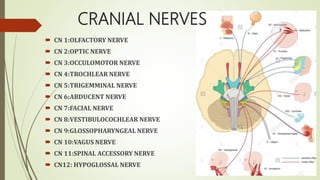
The cranial nerves control sensory and motor functions of the head and neck. There are 12 pairs of cranial nerves numbered I to XII. The document provides details of the origin, function and clinical evaluation methods for each cranial nerve including tests of sensory function, eye movements, facial expression, hearing and tongue movement.



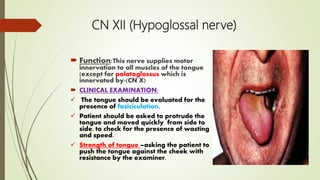
![ MOTOR FUNCTIONS:
Inspect for wasting of the temporal
and masseter muscles
Ask patient to clench their teeth and
palpate for contraction of the temporal
and masseter muscles
Ask patient to open their mouth and
hold it open while the examiner
attempts to force it shut [pterygoid
muscles].
JAW JERK TEST
Ask the patient to open her
mouth fully, and close
halfway place index finger
on her chin and tap with a
patella hammer, if jaw jerk
is highly exaggerated.](https://image.slidesharecdn.com/judeppt-181007142057/85/CRANIAL-NERVE-EXAMINATION-10-320.jpg)