Downloaded 178 times



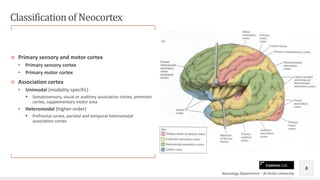




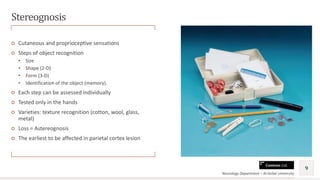







The document provides an overview of cortical sensations, detailing the posterior column and anterolateral pathways along with functionalities related to primary sensory and motor cortices. It discusses various types of sensory tests including stereognosis, graphesthesia, two-point discrimination, and sensory attention, along with the implications of impairments such as agnosia. Additionally, it emphasizes the importance of cortical regions in the recognition and interpretation of complex stimuli.










































![[Int. med] the sensory system from SIMS Lahore](https://cdn.slidesharecdn.com/ss_thumbnails/7xvc8ucgqb6ynpfpjojo-signature-b01672da1ecf8b94befb115319b147a085de390b8cb403389bce6c156545fbb5-poli-150815171700-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)












































