Downloaded 66 times

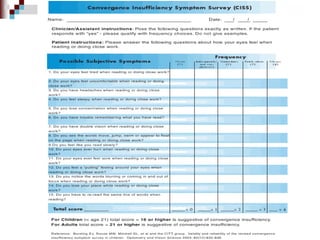
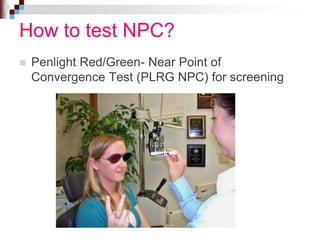

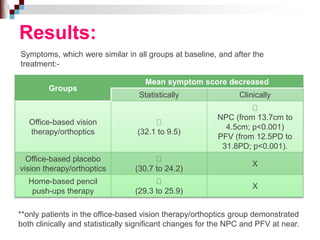




This document discusses convergence insufficiency (CI), a binocular vision problem characterized by an inability to converge the eyes or sustain convergence. CI causes symptoms like headaches, eye strain, and blurred vision during close work. The document summarizes a clinical trial finding that office-based vision therapy is an effective treatment for CI, improving symptoms and convergence measures, while home exercises and placebo therapy were less effective. It encourages optometrists to screen for CI using tests like near point of convergence, recognize symptoms, and inform patients that vision therapy can effectively treat this common problem.



![Types of pediatric contact lens [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/typesofpediatriccontactlensautosaved-200210123904-thumbnail.jpg?width=640&height=640&fit=bounds)






































































































