
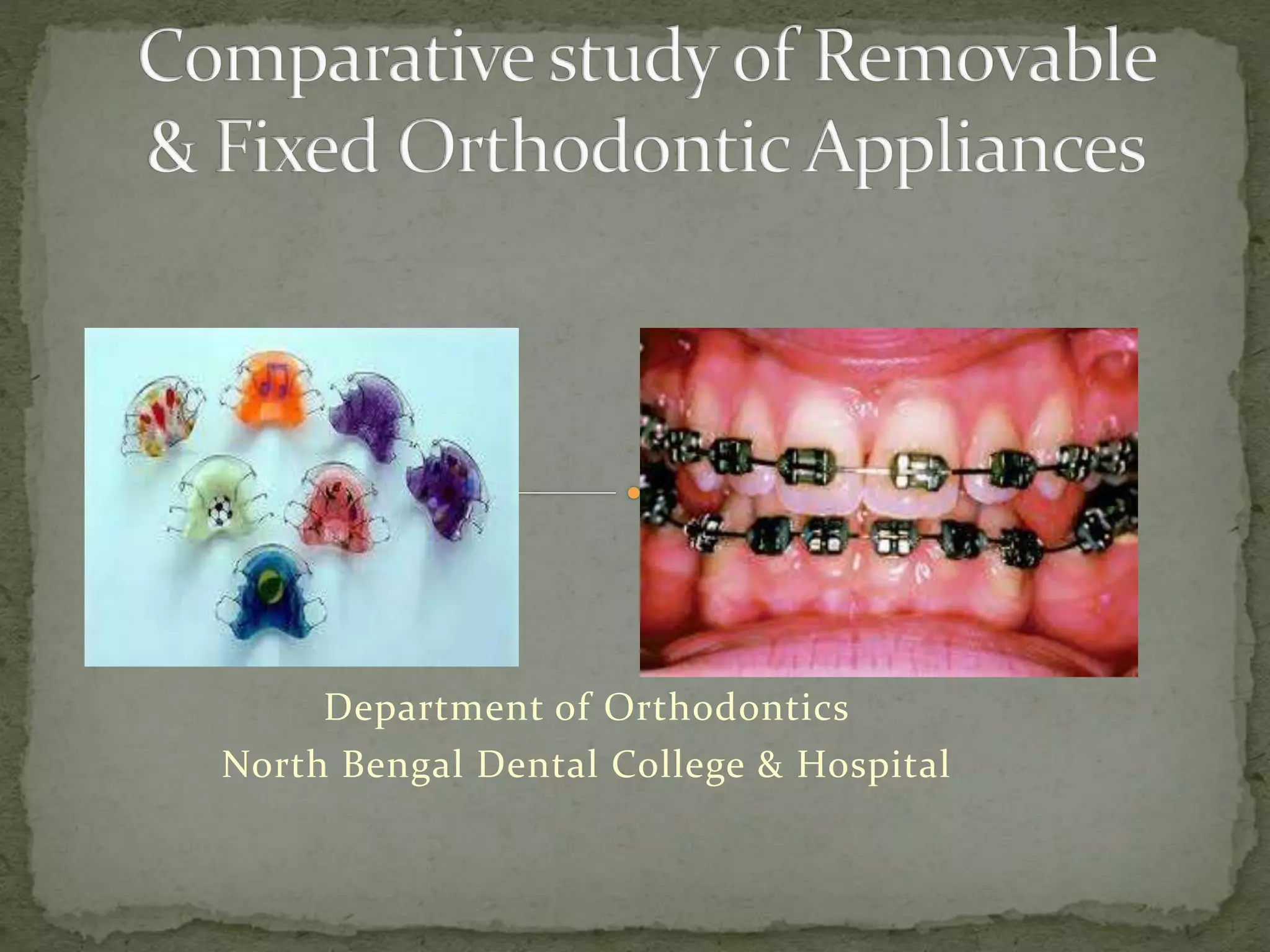



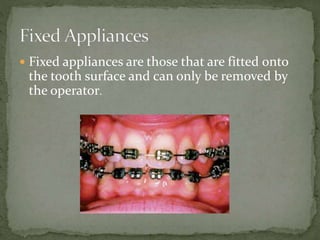
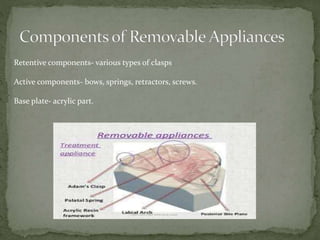
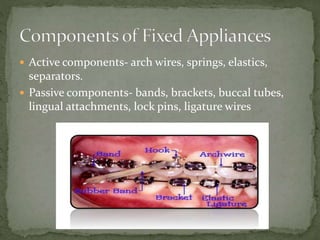
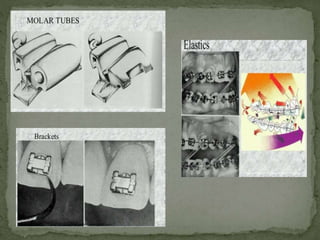
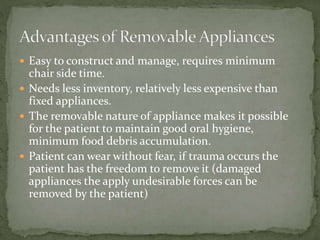
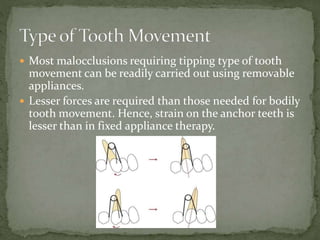
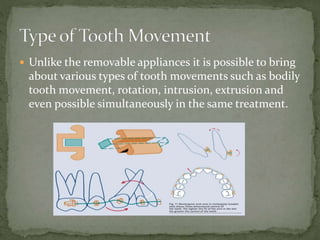
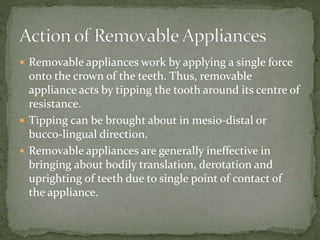
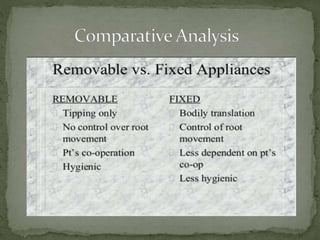



The document discusses removable and fixed orthodontic appliances. Removable appliances can tip teeth but cannot perform complex movements like fixed appliances. Removable appliances are easier to construct and manage, require less chair time, and allow for oral hygiene. However, they rely more on patient compliance and cannot move teeth as precisely as fixed appliances. While removable appliances can address mild to moderate malocclusions, fixed appliances offer better control and are needed for more complicated cases.













































![Removable Appliances ortho[Autosaved].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/removableappliancesautosaved-250321193254-b5973907-thumbnail.jpg?width=640&height=640&fit=bounds)








































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)














