Downloaded 1,391 times









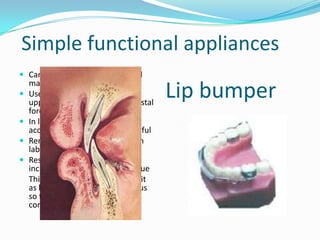
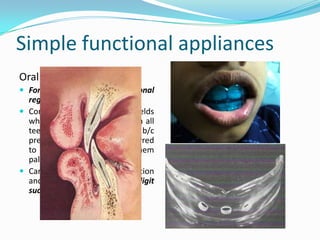





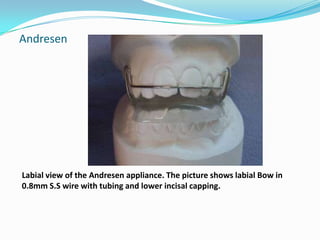
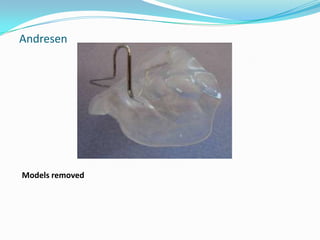
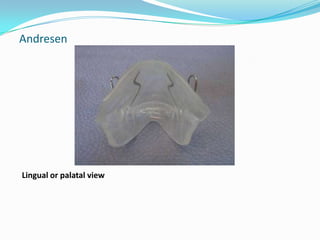

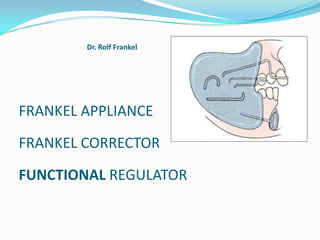
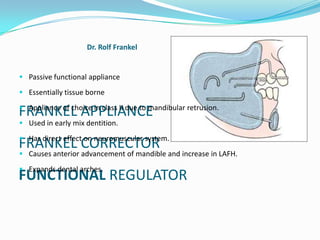











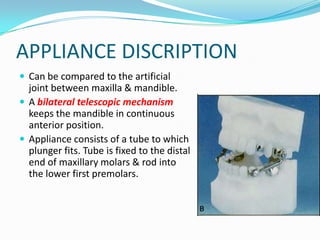
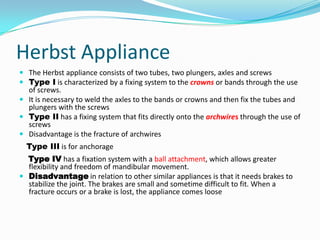


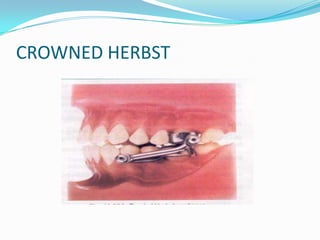





The document discusses different types of functional appliances used in orthodontics including simple functional appliances like lip bumpers and oral screens, as well as more complex removable appliances like the Frankel regulator, Bionator, activator, and twin block. It describes the indications, contraindications, components, and mechanics of several commonly used functional appliances. The document emphasizes that functional appliances aim to alter the neuromuscular environment and utilize muscle forces to effect skeletal and dental changes.



































































