

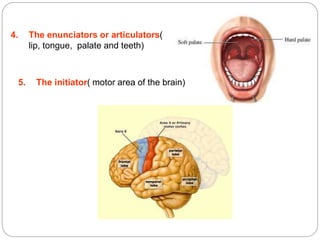



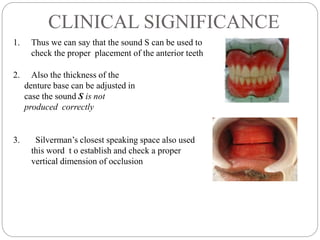








1. Phonetics refers to the sounds of speech and their production. Normal speech relies on the proper functioning of the lungs, vocal cords, oral cavity, and brain. 2. Consonant sounds are important for dentistry and can be classified based on their place of articulation. Sounds like S, T, and D involve the tongue and hard palate, while sounds like TH use the tongue and teeth. 3. Several aspects of denture design can affect speech, such as denture thickness, the vertical dimension of occlusion, and the positioning of teeth. For example, teeth that are too far back can cause difficulties producing F and V sounds. Phonetics is useful for evaluating denture fit























































































