Downloaded 35 times

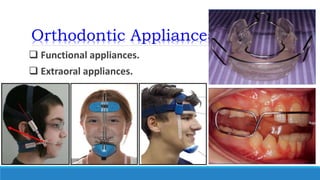




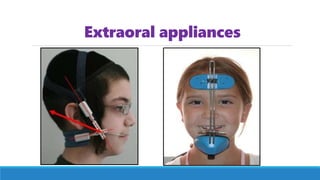


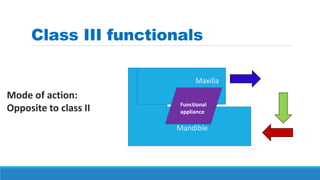
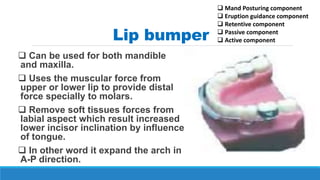
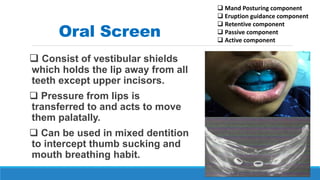
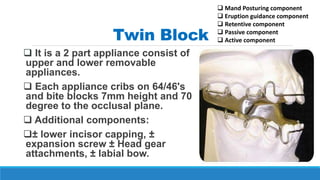


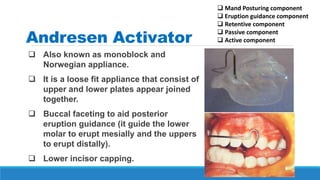
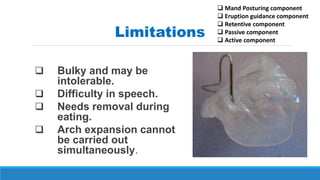
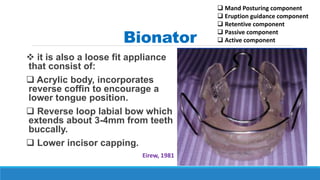
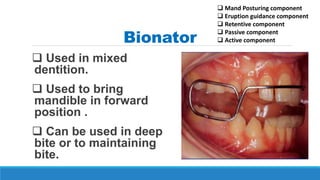
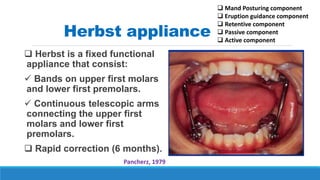
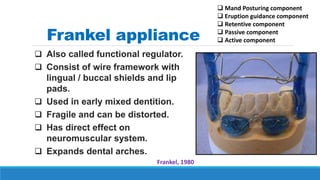

This document provides an overview of functional orthodontic appliances. It begins by explaining that orthodontic appliances can be either removable, fixed, or functional. Functional appliances work by utilizing forces from the muscles rather than having an active component themselves. They are often removable and used to treat Class II and Class III malocclusions in growing patients. Common functional appliances discussed include lip bumpers, oral screens, twin blocks, Andresen activators, Bionators, Herbst appliances, and Frankel regulators. The document concludes by discussing considerations for choosing a functional appliance and their management.























































































