Downloaded 3,850 times











































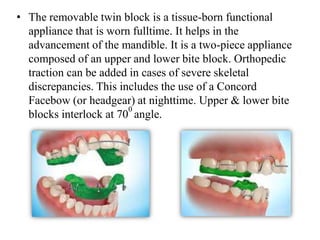















This document provides an overview of functional appliances used in orthodontic treatment. It begins with definitions of functional appliances and a brief history of their development. It then discusses the basis, classification, forces, treatment principles, indications, actions, case selection, and common appliances like the activator, frankel regulator, bionator, twin block, and Herbst appliance. It provides details on their design, indications, mode of action, and advantages. In summary, the document serves as a comprehensive guide to functional appliances, their development and use in orthodontic treatment.










































































