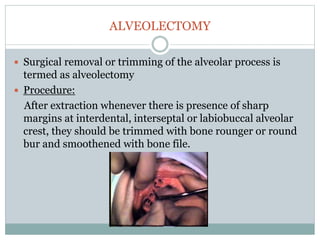



Pre-prosthetic surgery is essential for patients who cannot effectively use dentures due to issues like bone atrophy and localized tissue problems. The surgery aims to modify hard and soft tissues to facilitate the fitting of prosthetics while ensuring stability and retention. Key procedures include alveolectomy, alveoloplasty, and various other surgeries to address bone and soft tissue deformities, tailored to enhance patient comfort and prosthetic success.






















































































