The document provides an overview of fixed orthodontic appliances, detailing their components, types, and techniques involved in tooth movement. It explains the effects of applying mild versus extreme forces on tooth and periodontal structures, defining optimum orthodontic forces and different types of tooth movements such as tipping, bodily movement, and torque. Additionally, the document outlines methods of appliance attachment including banding and bonding, and discusses the characteristics and advantages of various orthodontic materials used in fixed appliances.












































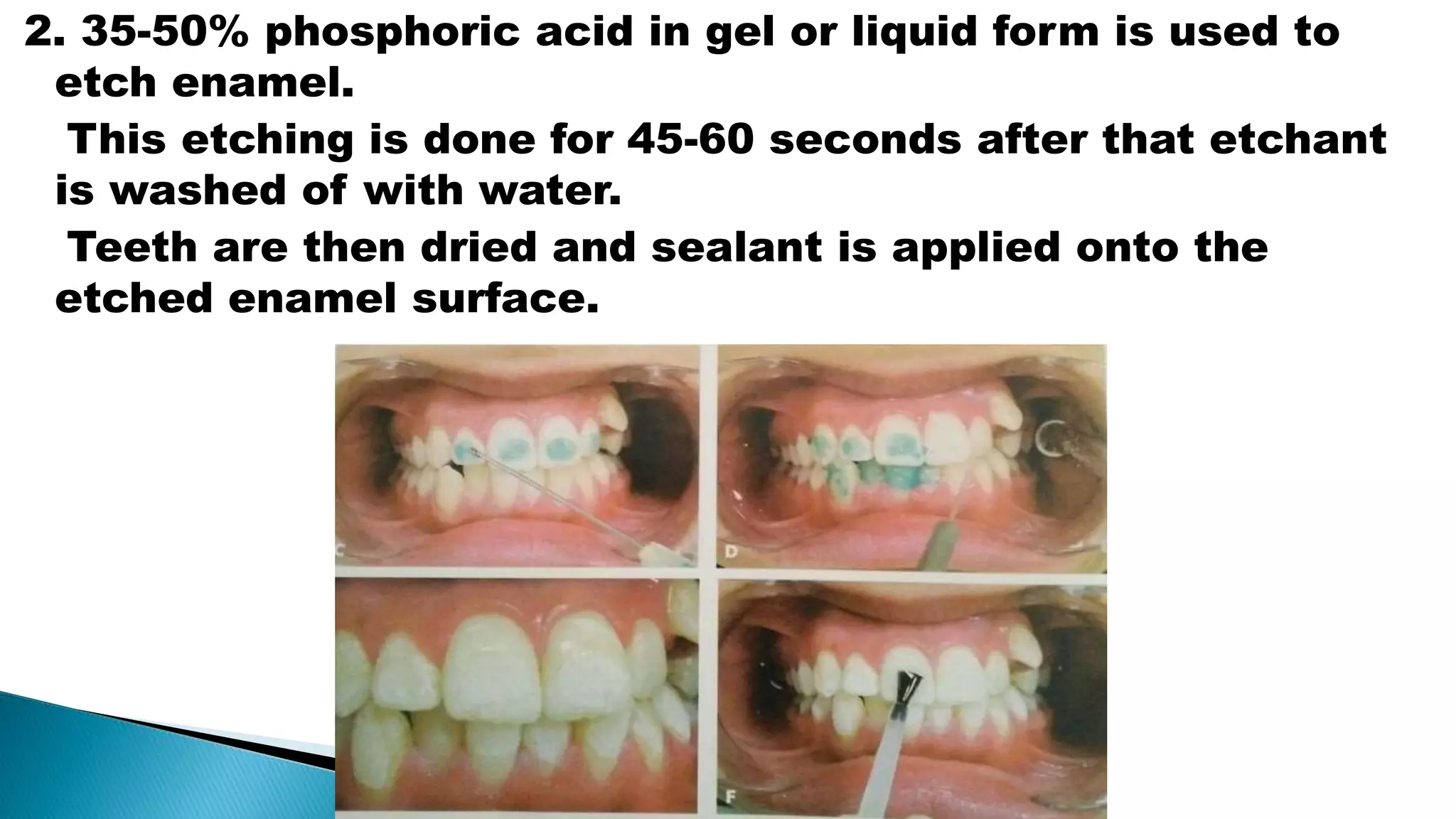
![2) Bonding:
The method of fixing attachments directly over the enamel
using adhesive resins is called bonding
Introduced by buonocore. [ in 1955 ]](https://image.slidesharecdn.com/orthodonticfixedappliances-171127063225/75/Orthodontic-fixed-appliances-68-2048.jpg)







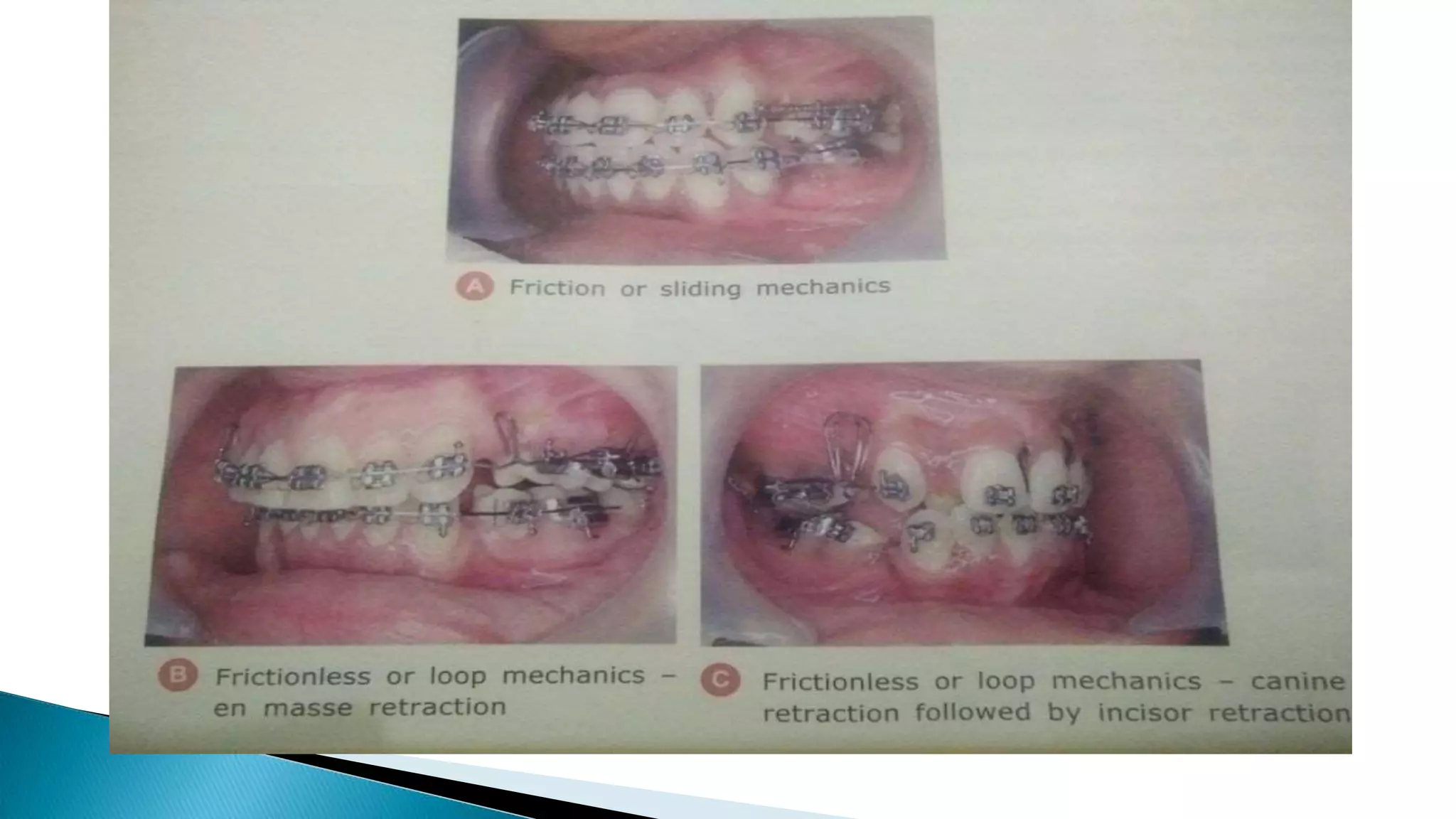
![1. Friction or sliding mechanisms:
After proper alignment of the bracket [teeth], arch wire
easily slides through the buccal tube.
Rectangular stainless steel wire with 0.18’’ * 0.025’’ or
0.019’’ * 0.025’’ dimension are used for the purpose of
anterior retraction.](https://image.slidesharecdn.com/orthodonticfixedappliances-171127063225/75/Orthodontic-fixed-appliances-82-2048.jpg)