






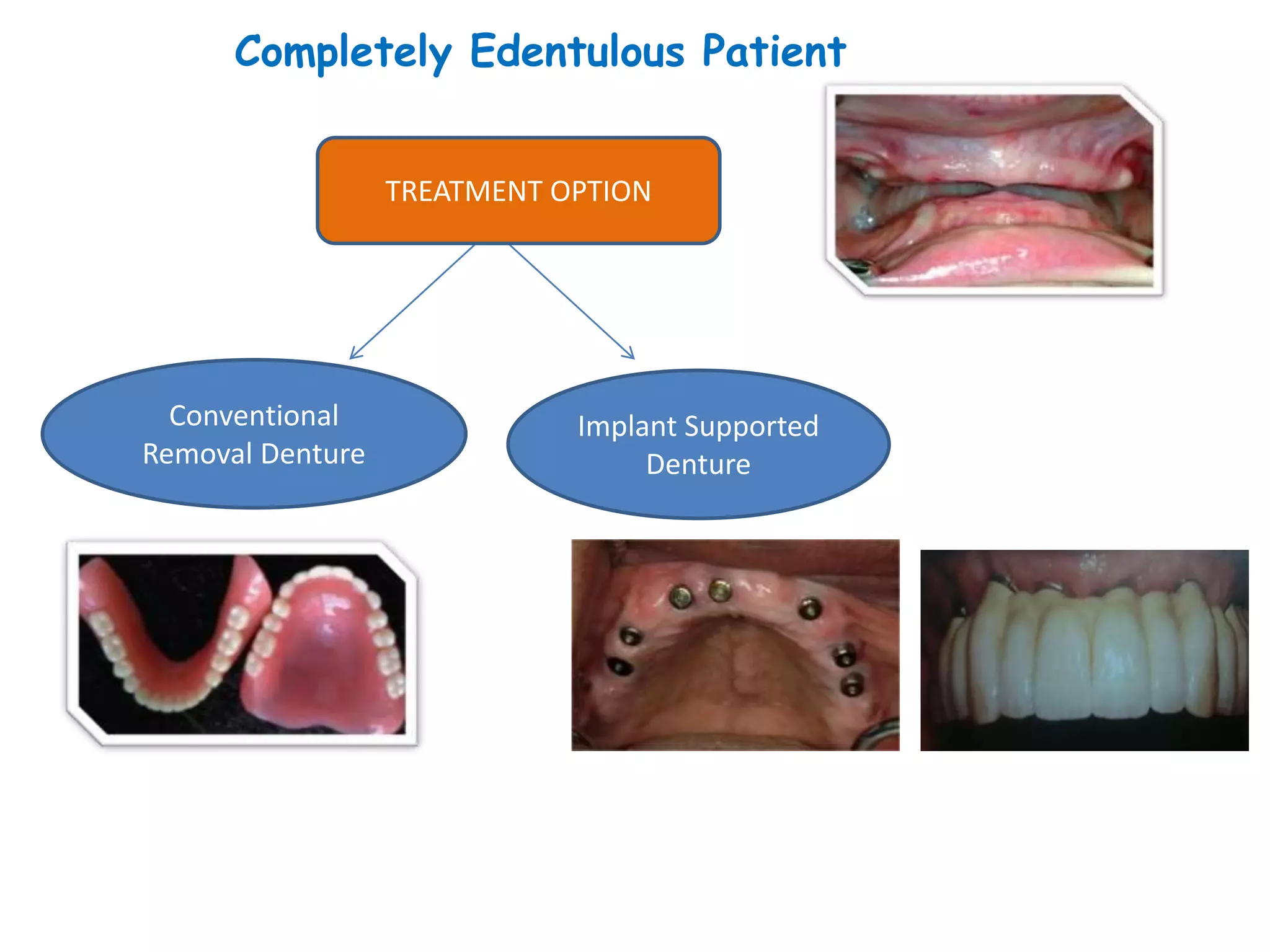















































































Implants can provide support and retention for fixed or removable prostheses. There are various types of implants classified based on location and surgical exposure. Osseointegration is the key mechanism for implant integration with bone. Implants are indicated for fully and partially edentulous patients to improve function, aesthetics and quality of life over conventional dentures. Treatment options include implant overdentures, fixed bridges and single tooth implants. Masticatory performance is improved with implant supported or retained dentures compared to conventional dentures.























































































