Downloaded 40 times
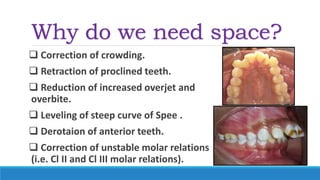
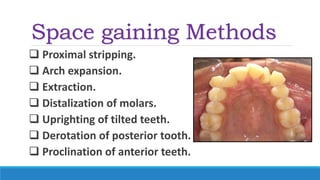
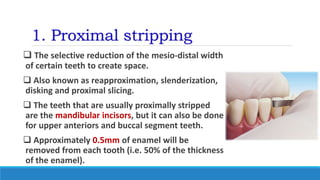
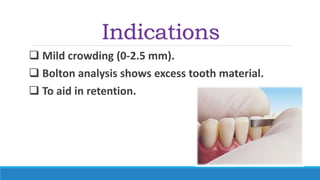

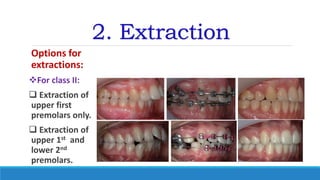
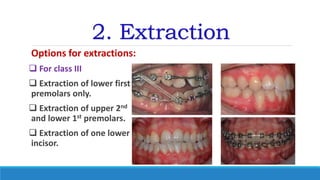
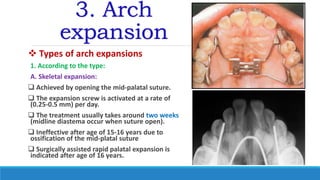
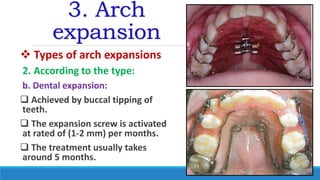
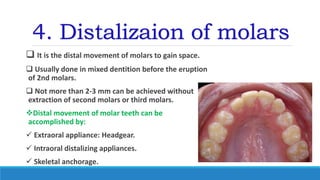

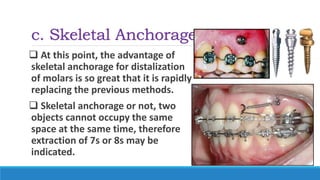
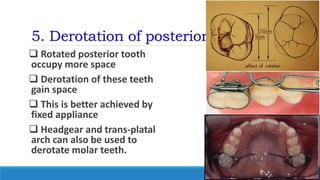
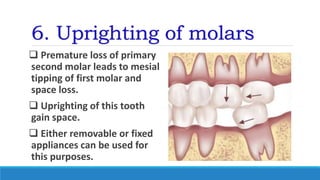
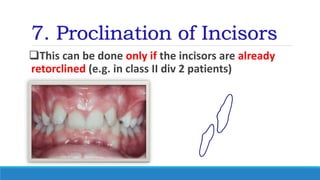

The document discusses various methods for gaining space in orthodontics, including proximal stripping, extraction, arch expansion, distalization of molars, derotation and uprighting of teeth, and proclination of incisors. Each method is explained with indications, advantages, and disadvantages, along with specific techniques and appliances used. The author emphasizes the importance of these methods in correcting dental crowding and improving overall dental alignment.