Downloaded 306 times


































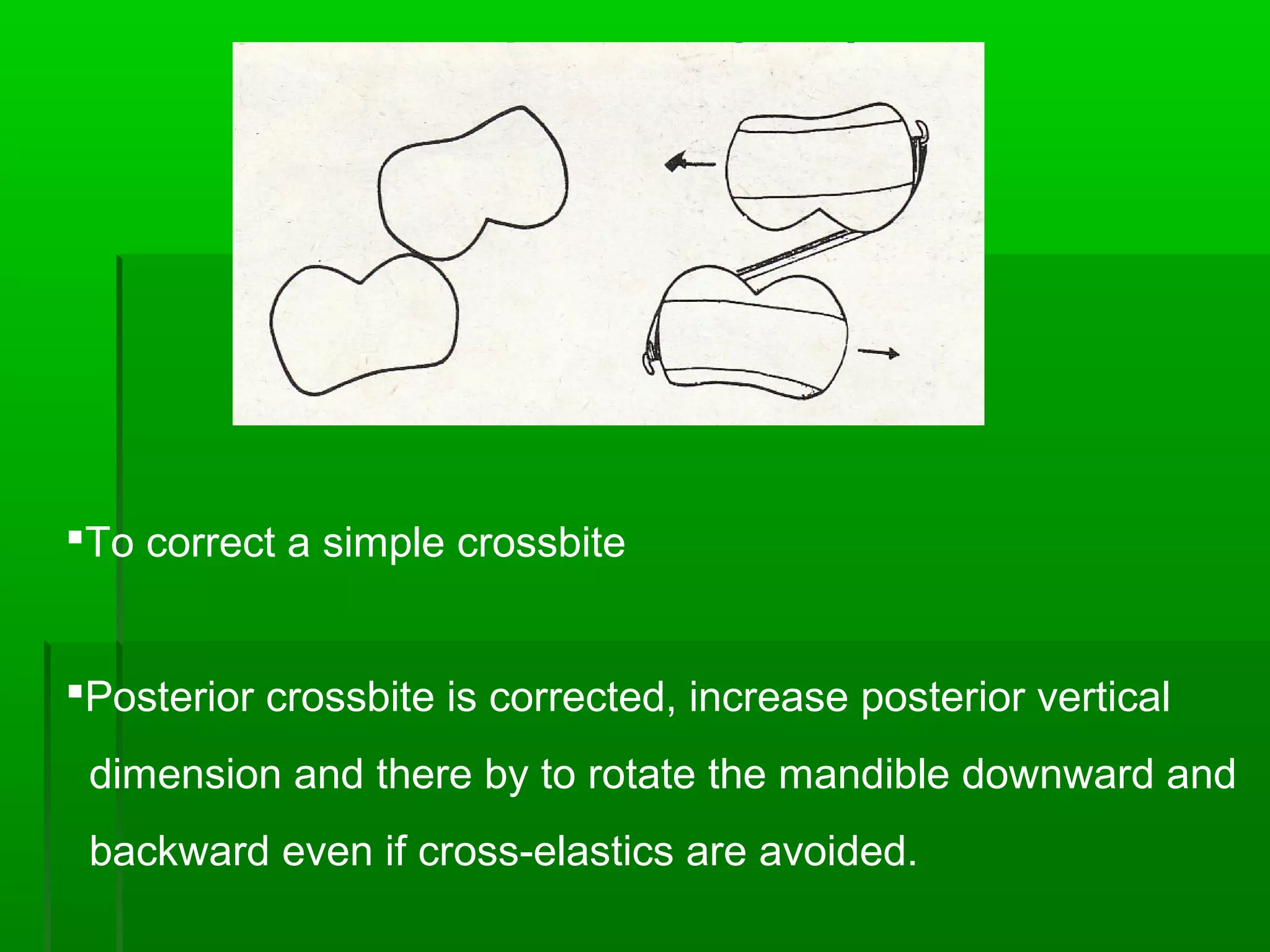
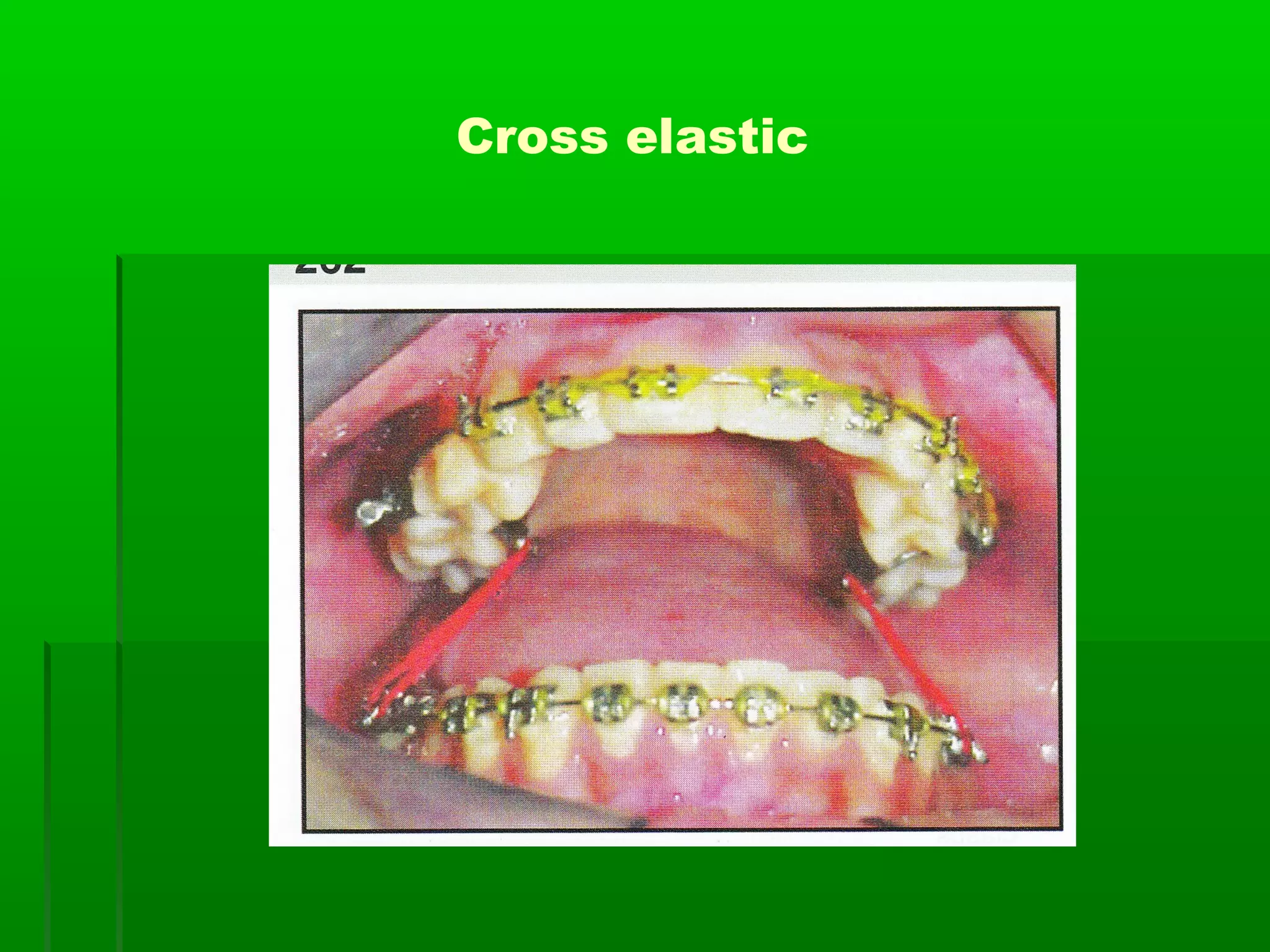
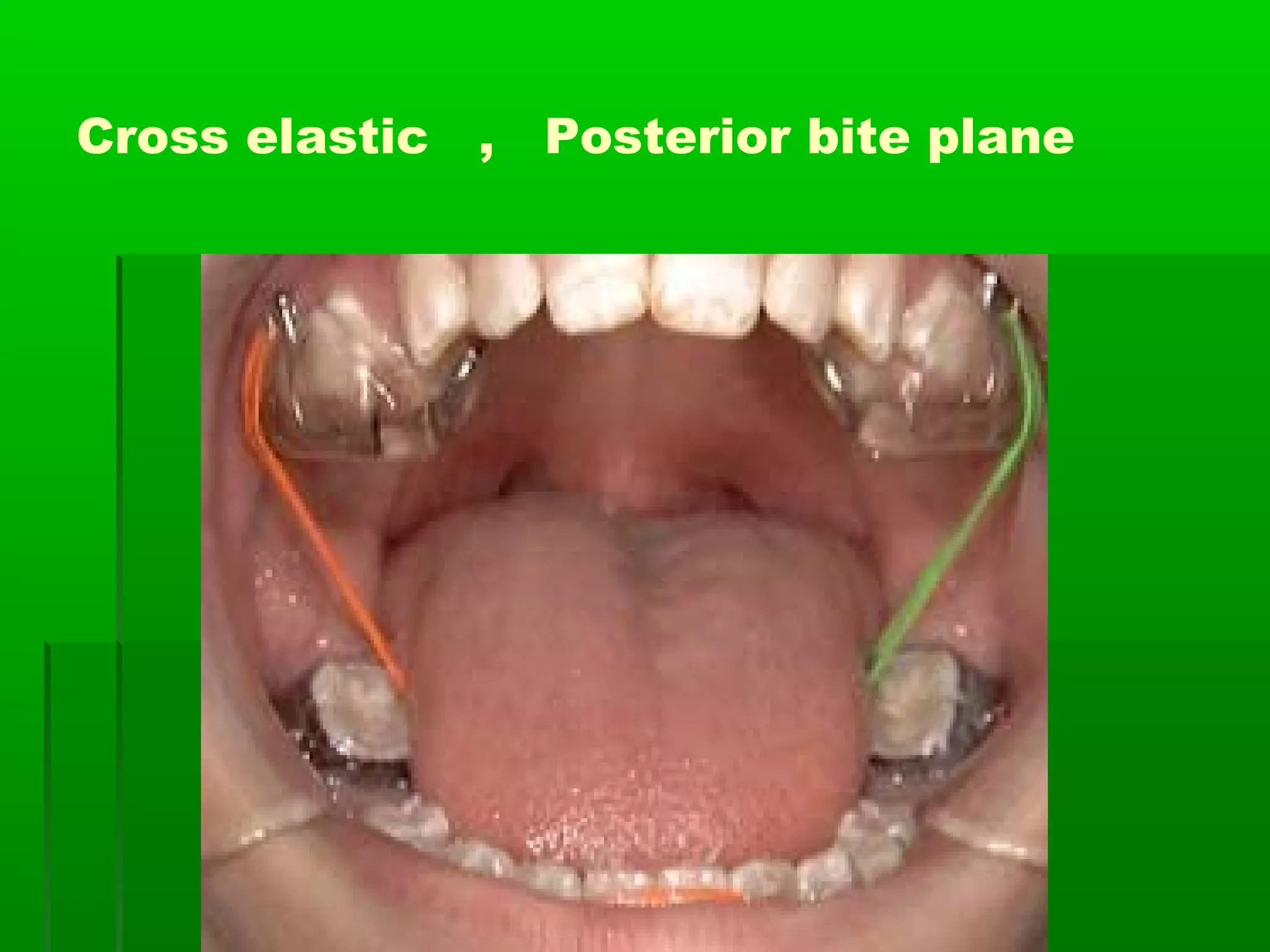








Posterior crossbite can be caused by skeletal factors like a narrow maxilla or wide mandible, or dental factors such as teeth erupting in the wrong position. Treatment depends on the cause, but may involve rapid or slow palatal expansion using appliances to widen the maxilla. For skeletal crossbites, expansion appliances are cemented and activated to apply force across the midpalatal suture. For dental crossbites, lighter forces from things like elastic threads or springs are used to move individual teeth. Crossbites caused by jaw shifting are treated by eliminating interferences and expanding a narrow arch. Habit-induced crossbites are addressed by treating the underlying habit. Correcting crossbites early in the























































































