Cobalamin (vitamin B12) is an essential water-soluble vitamin that contains cobalt. It is involved in two important reactions in the human body: the conversion of homocysteine to methionine, and the conversion of methylmalonyl CoA to succinyl CoA. Vitamin B12 deficiency can cause megaloblastic anemia and neurological problems due to the impaired function of these two reactions. Diagnosis involves blood tests to measure vitamin B12 levels as well as metabolic biomarkers like methylmalonic acid.
Introduction to Cobalamin, presented by Gandham Rajeev from Akash Institute, Bangalore.
Cobalamin as the extrinsic factor and its chemical structure, highlighting cobalt content and corrin ring.
Different forms of Vitamin B12: Cyanocobalamin, Hydroxycobalamin, Methylcobalamin, and Adenosyl cobalamin.
Vitamin B12 release from food, combined with intrinsic factor, absorption in the ileum, and transportation in blood.
Enzymes requiring Vitamin B12 for biochemical reactions, including conversion of homocysteine to methionine.
Effects of Vitamin B12 deficiency resulting in methyl folate trap, impacting nucleic acid synthesis.
Methylmalonyl CoA mutase reaction and consequences of Vitamin B12 deficiency leading to methylmalonic aciduria.
Sources of Vitamin B12 mainly from animal products, with recommended daily intake for different demographics.
Consequences include megaloblastic anemia, gastrointestinal dysfunction, neurological issues, and clinical signs.Diagnostic tests for Vitamin B12, including serum B12 levels, methylmalonic acid excretion, and Schilling test.
List of references used in the presentation, including biochemistry and clinical chemistry textbooks.
COBALAMINE (B12]
Gandham. Rajeev
Departmentof Biochemistry,
Akash Institute of Medical Sciences
& Research Centre,
Devanahalli, Bangalore,
Karnataka, India.
E-Mail: gandhamrajeev33@gmail.com
3.
Cobalamin
Extrinsicfactor (EF) of castle
Antipernicious anemia factor
Chemistry:
Vitamin B12 is water soluble, heat stable and red
in color
It contains 4.35% cobalt by weight
Four pyrrole rings co-ordinated with a cobalt
atom is called as a Corrin ring
4.
The corrinring has four pyrrol units, like porphyrin
Two of the pyrrole units (A&D) are directly bound
to each other where as the other two (B & C) are
held by methene bridges
The groups namely methyl, acetamide and
propionamide are the substituents on the pyrrole
rings
Cobalt present at the centre of the corrin ring is
bonded to the four pyrrole nitrogens
5.
Cobalt alsoholds dimethyl benzimidazole (DMB)
containing ribose 5-Phosphate and amino
isopropanol
A nitrogen atom dimethyl benzimidazole is
linked to cobalt
The amide group of aminoisopropanol binds with
D ring of corrin
The cobalt atom also possesses a sixth
substituent group located above the plane of the
corrin ring
All theforms of vitamin B12 are called cobalamins
because of the presence of cobalt atom
Different forms of cobalamins include
Cyanocabalamin:- It refers to the isolated form of
vitamin B12 in which cyanide was added to
promote crystallization of cobalamin during the
isolation process
Hydroxycobalamin:- It was usually present in the
tissues and in the naturally occurring forms of
Vitamin B12
9.
Methylcobalamin :-Methyl group replaces
adenosyl group
Adenosyl cobalamin (Ado-B12):-
When taken up by the cells, these groups are
removed and deoxy adenosyl cobalamin or Ado-
B12 is formed
10.
In thefood, vitamin B12 is present as a complex
with proteins
The free form of vitamin B12 is released by
cooking, HCL present in gastric juice and
proteolysis by pepsin in the stomach
Mechanism:-
The absorbance of vitamin B12 requires intrinsic
factor
Intrinsic factor is a glycoprotein secreted by parietal
cells of stomach
11.
Vitamin B12combines with intrinsic factor
The vitamin B12 – intrinsic factor complex reaches
the ileum where it is absorbed
In the ileum, the complex attaches to a specific
receptor and is taken up by the mucosal cell.
In the mucosal cell, vitamin B12 is released from
its complex and reaches the portal circulation
12.
In theportal blood, it is transported in combination
with transcobalamin II
Vitamin B12 is presented to cells where it is taken
up by the cells through receptor mediated
endocytosis
Storage:
It is mainly stored in liver, leukocytes and gastric
mucosa
It is stored as complex with transcobalamin-I&II
About 10enzymes requiring vitamin B12 have
been identified
Most of them are found in bacteria ( mutase,
ribonucleotide reductase, etc.)
There are two reactions in mammals that
dependent on vitamin B12
15.
Methyl cobalaminis essential for the conversion of
homocysteine to methionine and formation of FH4
from methyl FH4
The reaction is catalyzed by homocysteine methyl
transferase
Homocysteine
Homocysteine methyl transferase
Methionine
methylcobalamin
THFN5 methyl THF
16.
The circulatingmethyl FH4 is converted to FH4
FH4 is either used for storage as folylpolyglutamate
form or it is utilized for other reactions such as
formation of methylene FH4
Methyl folate trap:-
In B12 deficiency, impaired conversion of methyl
FH4 to FH4 results in accumulation of methyl
FH4 & is called as methyl folate trap
Methyl folate trap results in decreased availability of
FH4 & FH4 derivatives that are
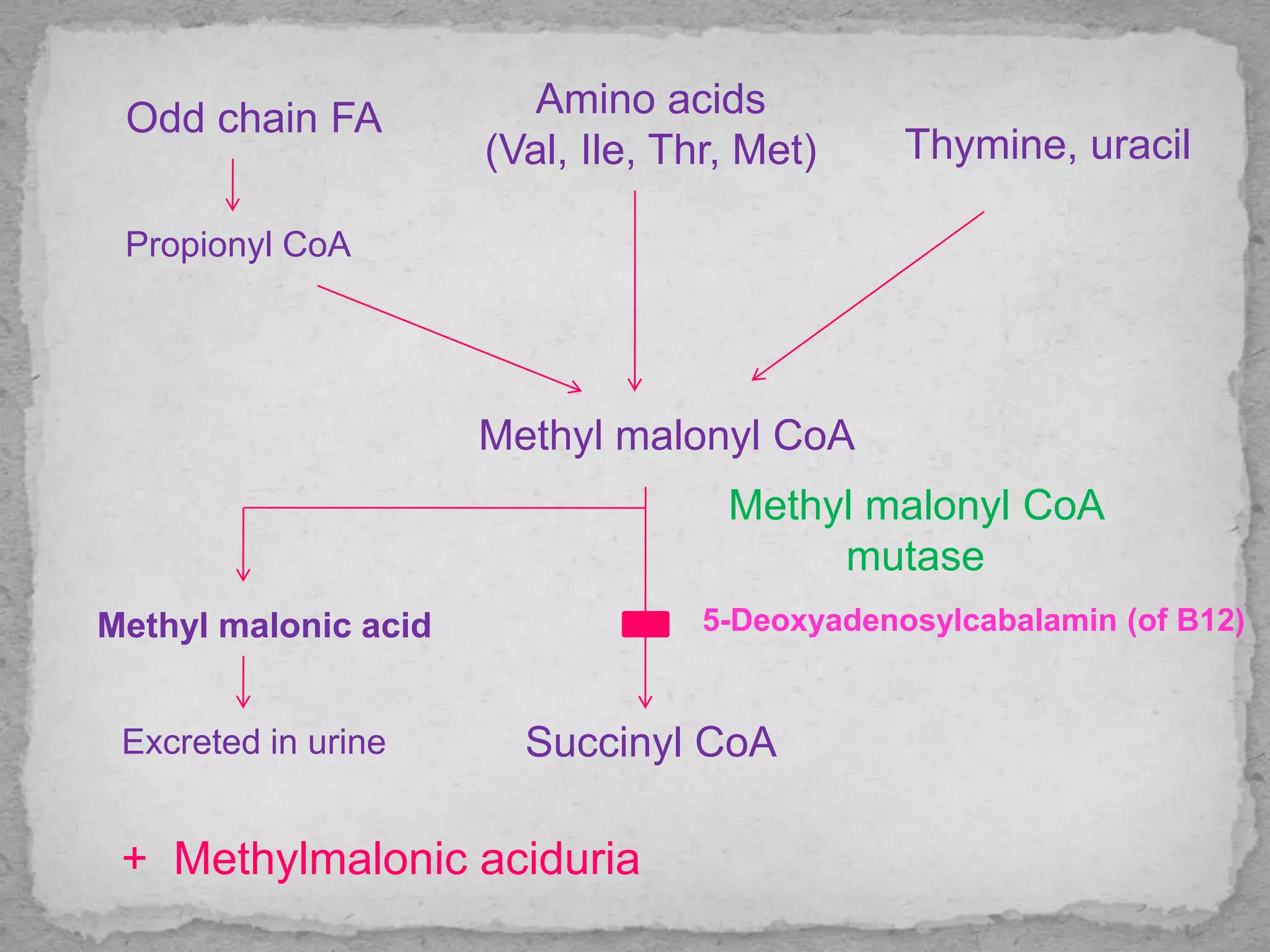
Isomerization ofmethyl CoA to succinyl CoA:-
The degradation of odd chain fatty acids and
some amino acids (valine, leucine etc) and
pyrimidines (thymine & Uracil) produce propionyl
CoA, an imp. Compound methylmalonyl CoA
The methyl malonyl CoA mutase converts methyl
malonyl CoA to succinyl CoA in the presence of
Vitamin B12,deoxyadenosyl cobalamin
20.
In B12deficiency, methyl malonyl CoA
accumulates and is excreted in urine as methyl
malonic acid
This condition is called as methylmalonic
aciduria, occurs in B12 deficiency.
Demyelination :- Myelination of nerves is impaired in
B12 deficiency due to accumulation of methylmalonyl
CoA
Demyelination is due excessive accumulation of
methylmalonyl CoA
21.
Odd chain FA
PropionylCoA
Amino acids
(Val, Ile, Thr, Met) Thymine, uracil
Methyl malonyl CoA
Succinyl CoA
Methyl malonyl CoA
mutase
Methyl malonic acid
Excreted in urine
5-Deoxyadenosylcabalamin (of B12)
+ Methylmalonic aciduria
22.
Rich sourcesof vitamin B12 are meats, egg, milk,
sea foods
B12 is synthesized by microorganisms
Vitamin B12 is not present in Plant sources
23.
Adults -1µg/day
Pregnancy & lactation -2 µg/day
Causes:
Inadequate intake-seen in pure vegetarians and
rarely in alcoholism
Impaired absorption
This is mainly caused by lack of intrinsic factor
Lack of intrinsic factor is called as pernicious
Deficiency
24.
anemia &it is caused by destruction of gastric
mucosa
Impaired absorption is also seen in small intestinal
disorders
Impaired storage and transport:
Inadequate utilization of vitamin occurs because of
liver diseases and abnormalities of transport
proteins
Increased requirements are seen in
hyperthyroidism, infancy & thalassemia
Increased excretion occurs in nephrotic syndrome
25.
Vitamin B12deficiency is characterized by
Megaloblastic anemia:
Feature of megaloblastic anemia include
pallor,fatigue, glossitis ( beefy red tongue) & slight
yellow discoloration of the conjunctiva due to
increased unconjugated bilirubin
Progression of anemia may result in angina &
congestive cardiac failure
27.
Gastrointestinal dysfunction:
GIT epithelial cells are undergoing rapid turnover
& dependent on vitamin B12
B12 deficiency results in weight loss & diarrhea
Demyelination of nervous tissue
Subacute combined degeneration:
Damage to nervous system is seen in B12
deficiency
28.
There isdemyelination affecting cerebral cortex as
well as dorsal column & pyramidal tract
Symmetrical paresthesia of extremities, alterations
of tendon & deep senses & reflexes, loss of
position sense, unsteadiness in gait, positive
Romberg’s sign & positive Babinski’s sign are
seen
Achlorhydria:
Absence of acid in gastric juice is associated with
B12 deficiency
29.
Serum B12:It is quantitated by radio-
immunoassay or by ELISA
Methyl melonic acid is excreted in urine
FIGLU excretion test
Peripheral smear: Peripheral blood & bone
marrow morphology shows magaloblastic anemia
Homocysteinuria: Excretion of homocysteine in
urine
30.
Schilling test:
Radioactive labelled (Cobalt-60) vitamin B12 1μ
g is given orally
In gastric atrophy cases, there is no absorption,
hence the entire radioactivity is excreted in faeces
& radioactivity is not observed in liver
If the cause is nutritional deficiency, there will be
increased absorption
Then radioactivity is noted in the liver region, with
very little excretion in feces
31.
Harper’s Biochemistry25th Edition.
Fundamentals of Clinical Chemistry by Tietz.
Text Book of Medical Biochemistry-A R Aroor.
Text Book of Biochemistry-DM Vasudevan
Text Book of Biochemistry-MN Chatterjea
Text Book of Biochemistry-Dr.U.Satyanarana
![COBALAMINE (B12]
Gandham. Rajeev
Department of Biochemistry,
Akash Institute of Medical Sciences
& Research Centre,
Devanahalli, Bangalore,
Karnataka, India.
E-Mail: gandhamrajeev33@gmail.com](https://image.slidesharecdn.com/12-161215122226/75/COBALAMINE-12-1-2048.jpg)