Download to read offline

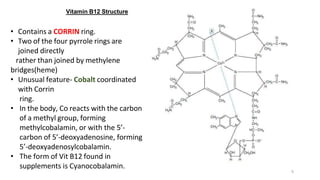
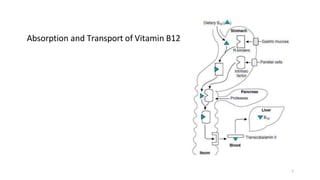

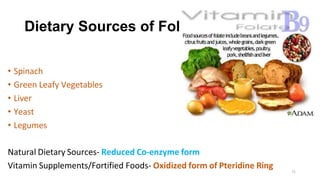
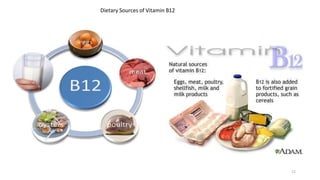










Folic acid and vitamin B12 are water soluble vitamins that play important roles in DNA synthesis and methylation reactions. Folic acid helps form red blood cells and genetic material, while vitamin B12 is involved in myelin production for nerve cells. Deficiencies can cause megaloblastic anemia and neurological issues. Dietary sources include leafy greens, liver, and fortified foods. Absorption involves conjugation and binding proteins, with metabolism intertwined between the vitamins. Testing of blood levels aids diagnosis of deficiency diseases.

































![GROUP_9_BIOCHEMISTRY PRESENTATION_FINAL[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/group9presentationfinal1-250912055037-2f32f493-thumbnail.jpg?width=640&height=640&fit=bounds)































