Downloaded 498 times

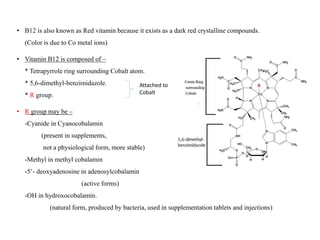
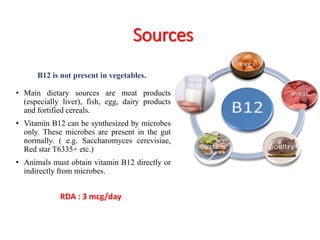
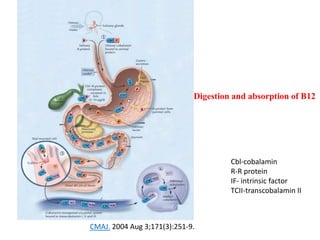
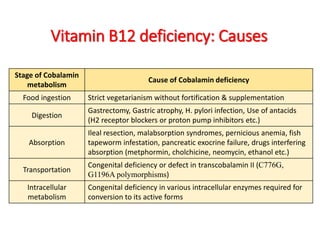
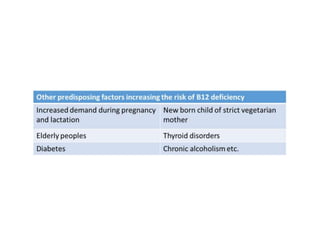
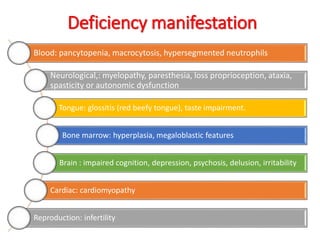
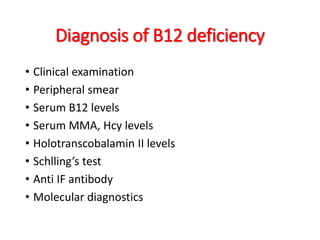


Vitamin B12, known as red vitamin, exists in various forms and is essential for multiple bodily functions, including DNA synthesis and neurological health. It is primarily sourced from animal products, and deficiencies may lead to significant health issues such as anemia, neurological disorders, and increased risk of osteoporosis and heart disease. Genetic factors can affect its metabolism and absorption, necessitating careful monitoring and potential supplementation, while long-term usage raises concerns over cancer risks.










![VITAMIN B12[CYNACOBALAMIN][COBALAMIN],SOURCES OFVITAMIN B12,VITAMIN B12 DEFIC...](https://cdn.slidesharecdn.com/ss_thumbnails/vitaminb12ravisankar-vignanpharmacy-130615121944-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)









































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)









