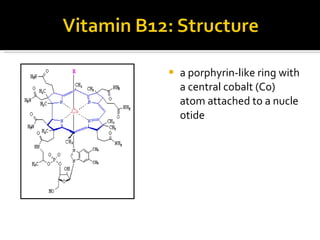
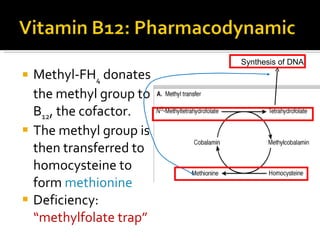
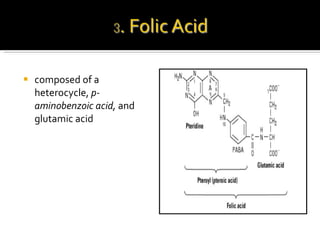
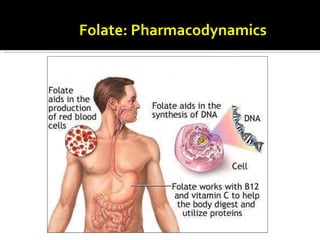
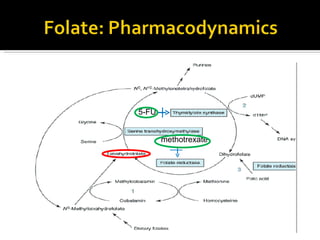
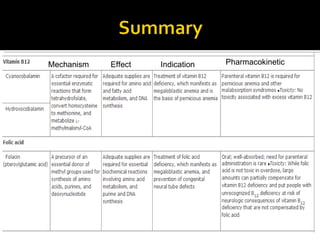
Vitamin B12 and folic acid are important hematinic agents that play critical roles in DNA synthesis and the methylation cycle. Vitamin B12 requires intrinsic factor for absorption in the terminal ileum and deficiency can lead to megaloblastic anemia or neurological issues. Folic acid deficiency is more common and can cause megaloblastic anemia, though it will not cause neurological problems like B12 deficiency. Both vitamins are important to replace through diet or supplements in various clinical populations.