The document provides an overview of spinal anatomy including:
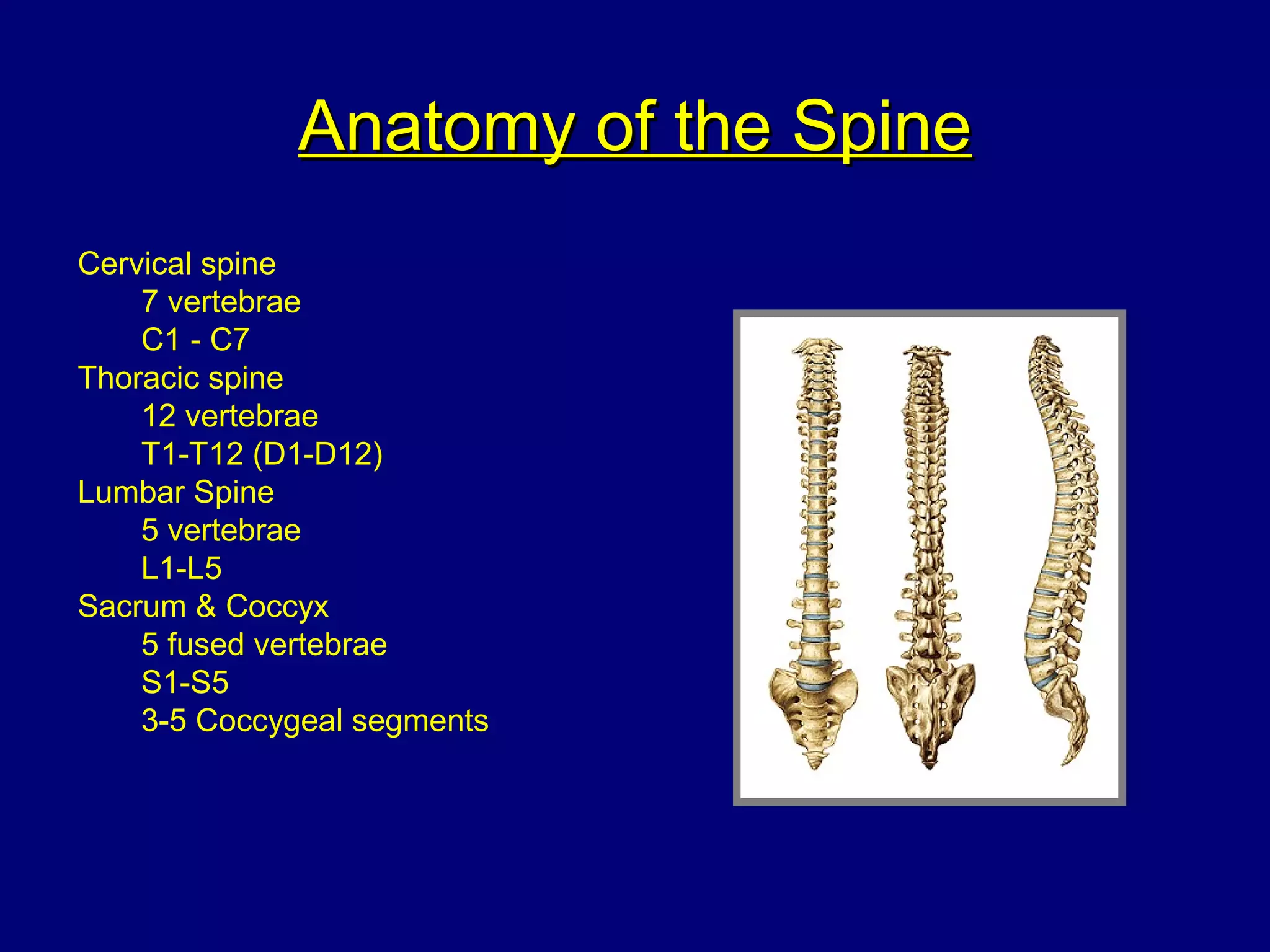
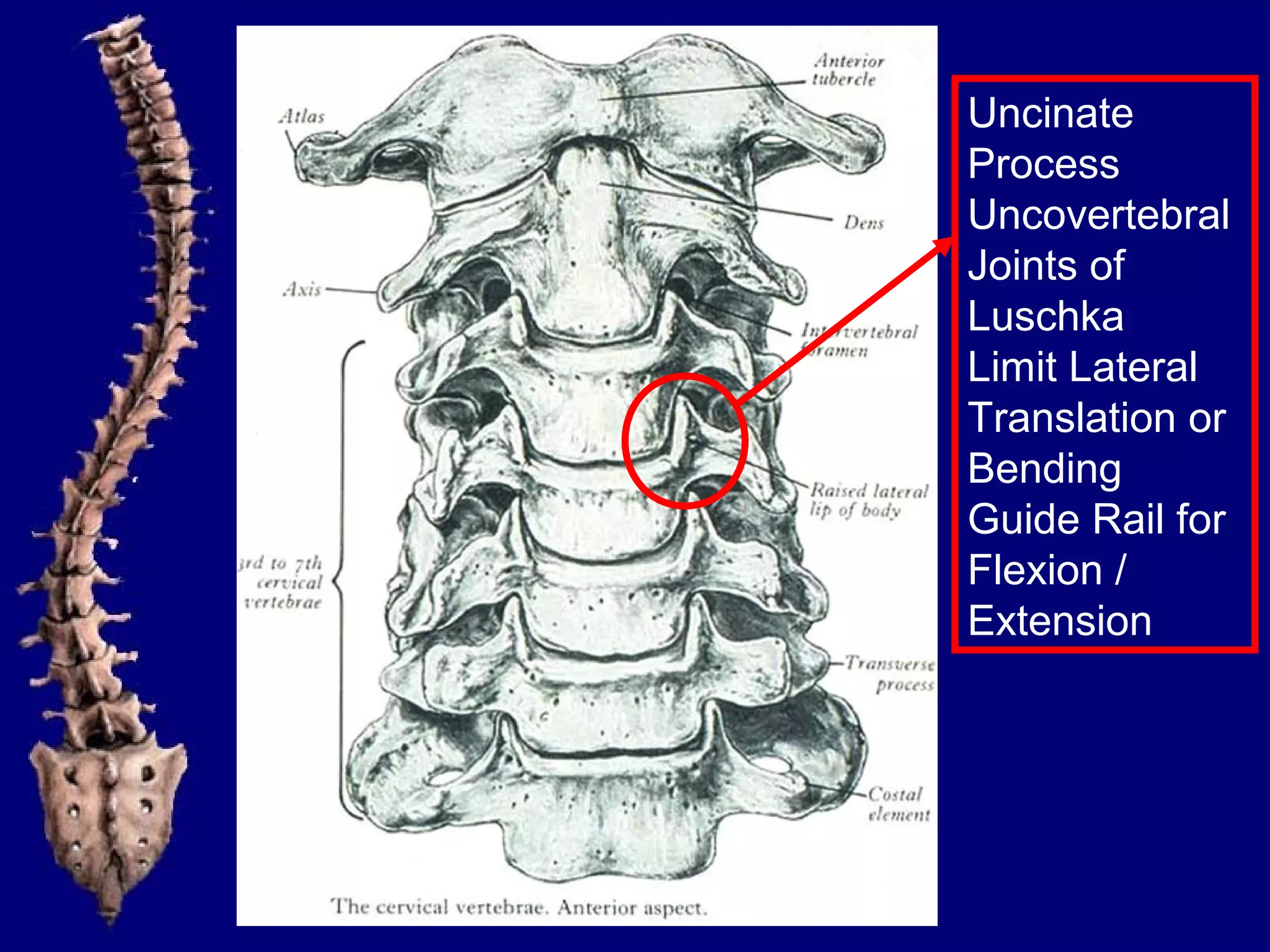
- The 7 cervical, 12 thoracic, 5 lumbar vertebrae and sacrum/coccyx bones that make up the spine.
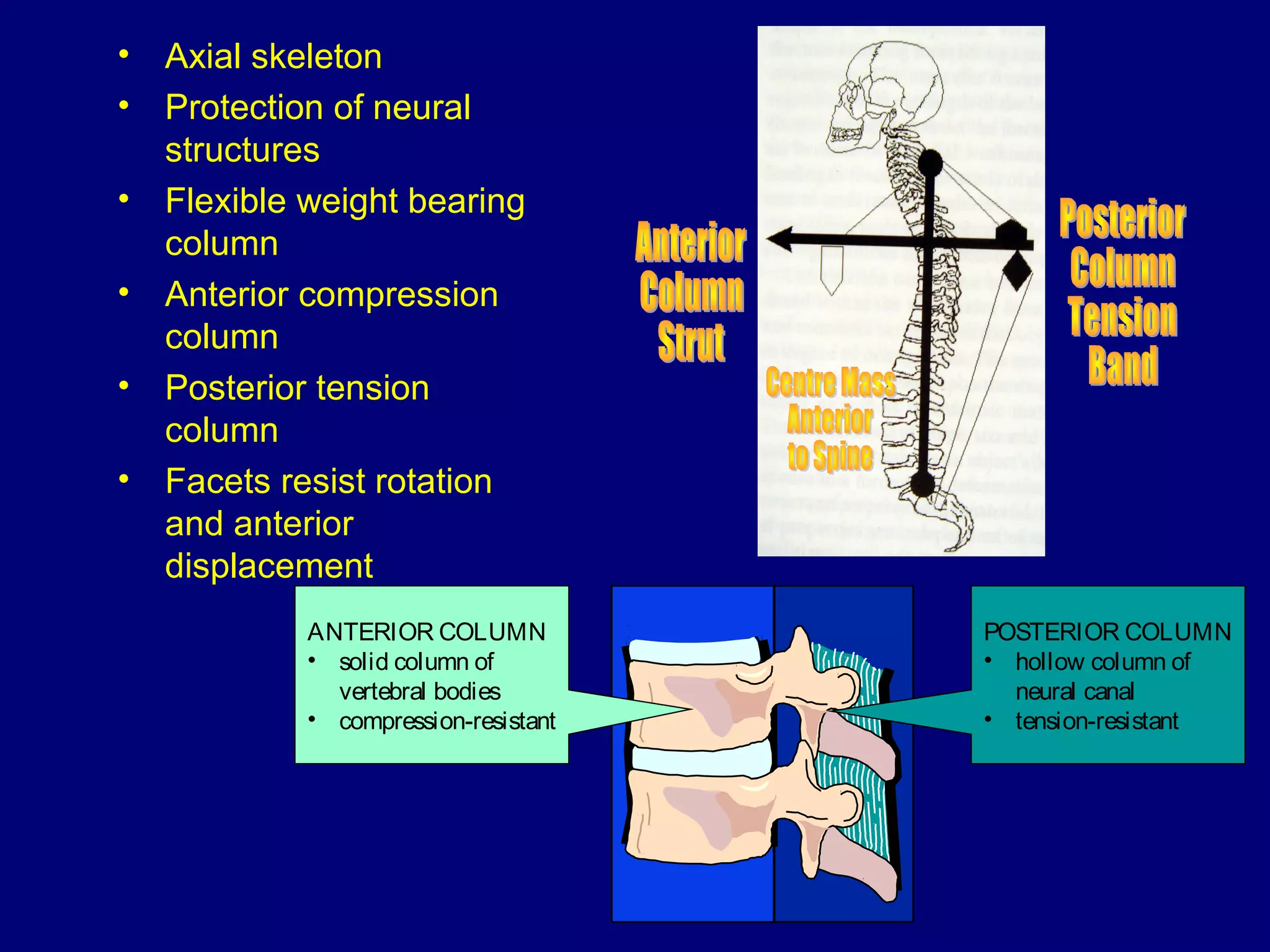
- Key structures like the anterior/posterior columns that provide compression/tension resistance.
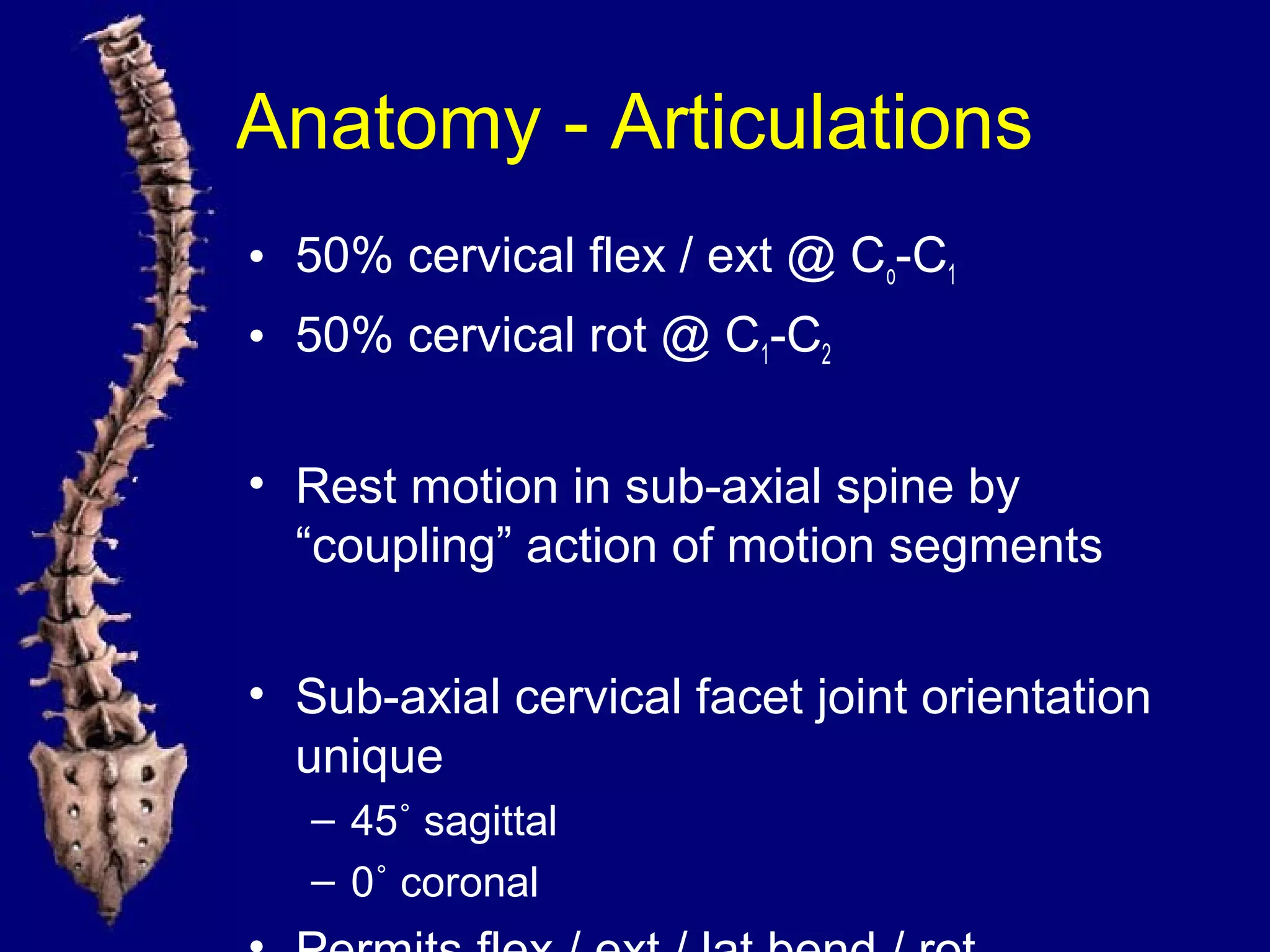
- Facet joints that resist rotation and displacement.
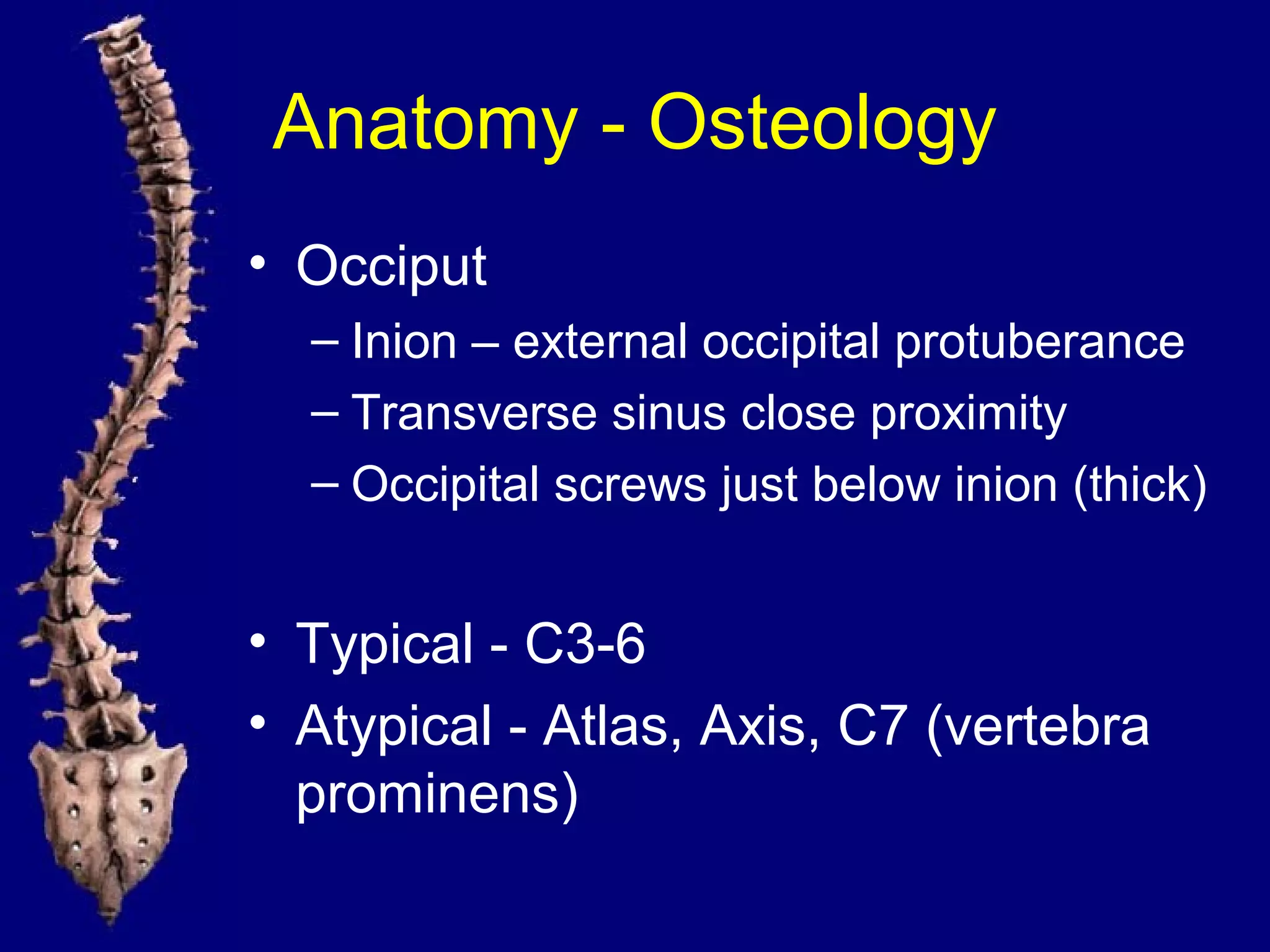
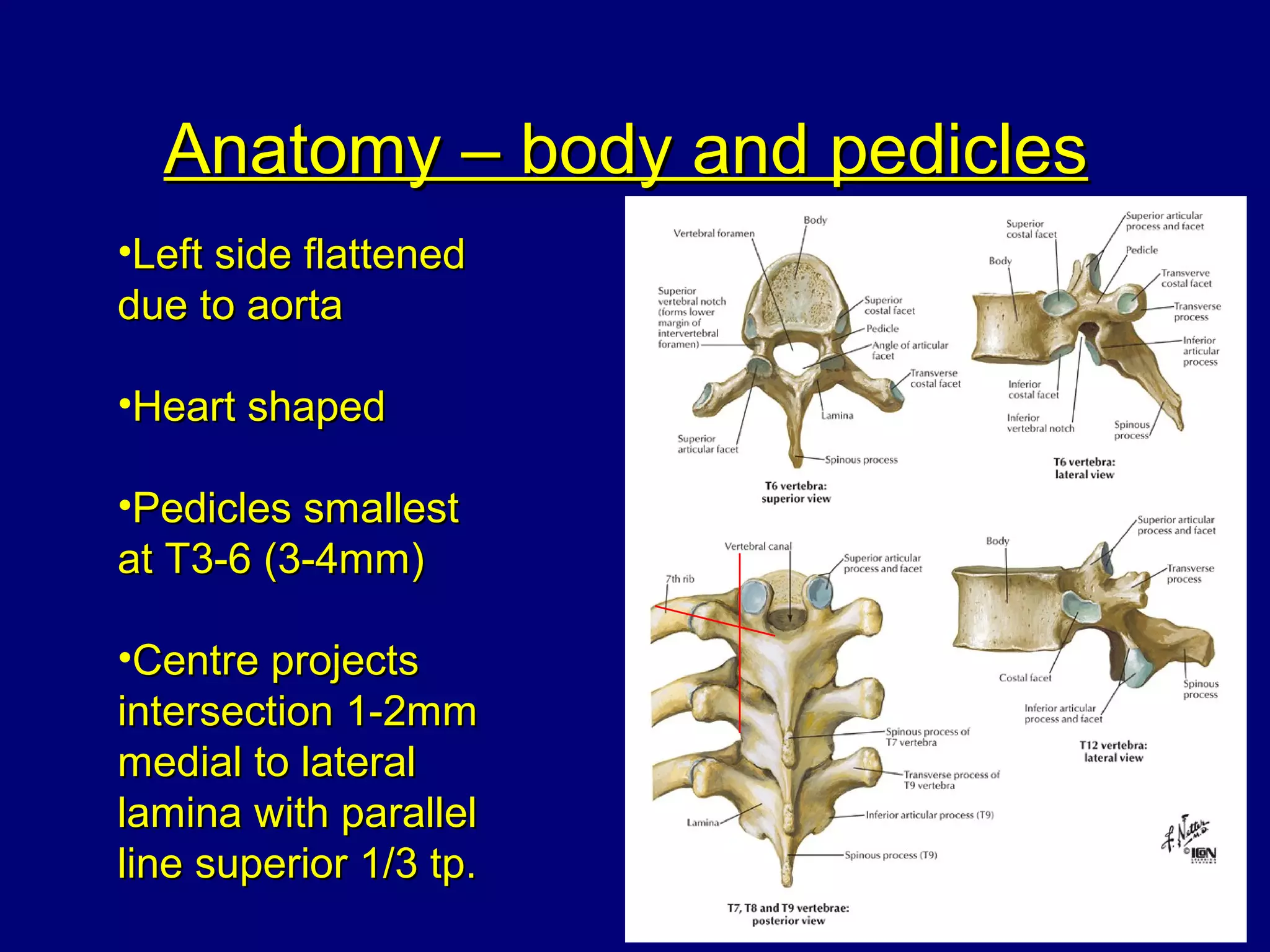
- Important anatomical features of each region like the cervical facet orientation and thoracic transverse processes.
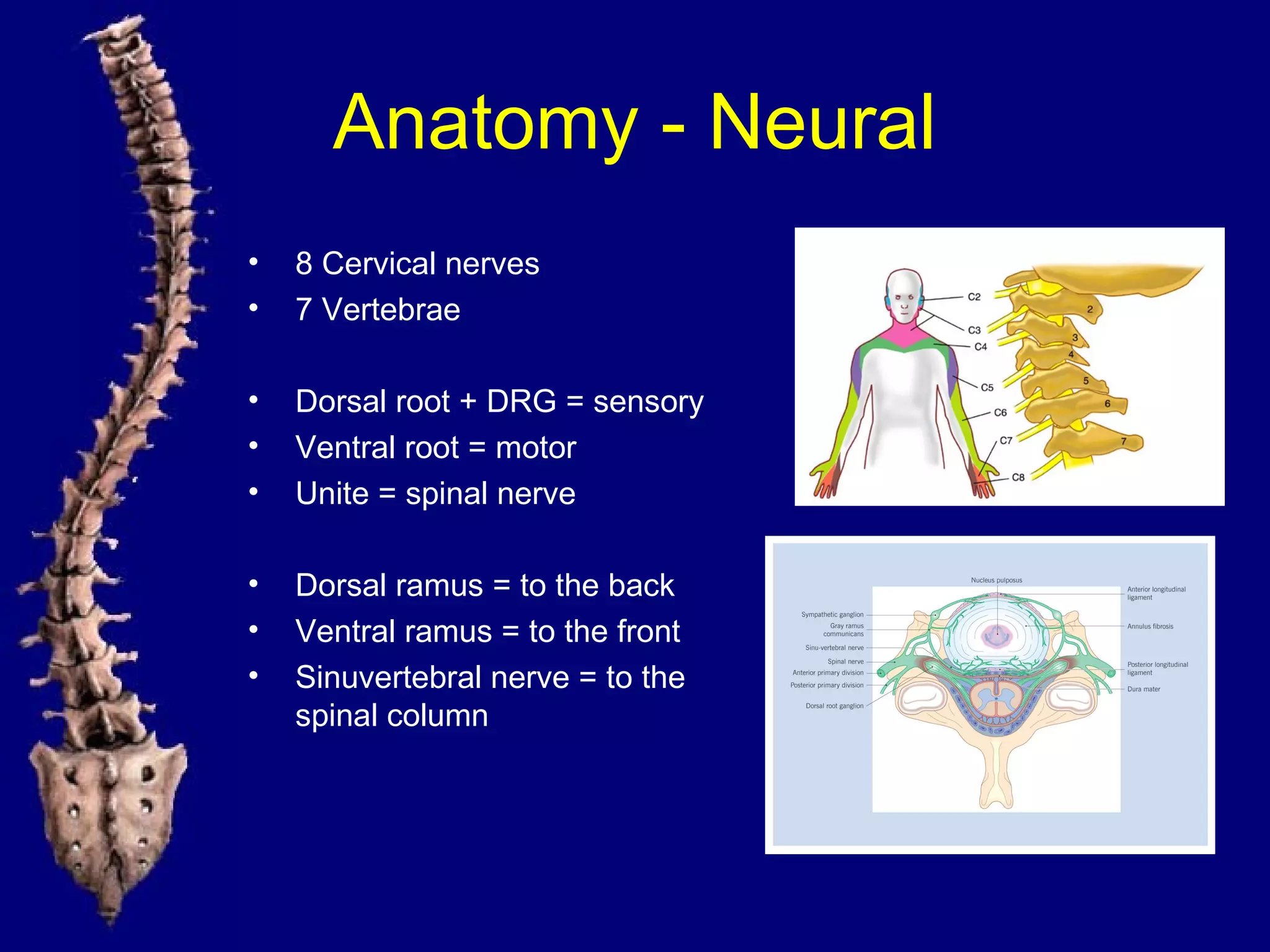
- Neural structures like the spinal cord, nerves and nerve roots.
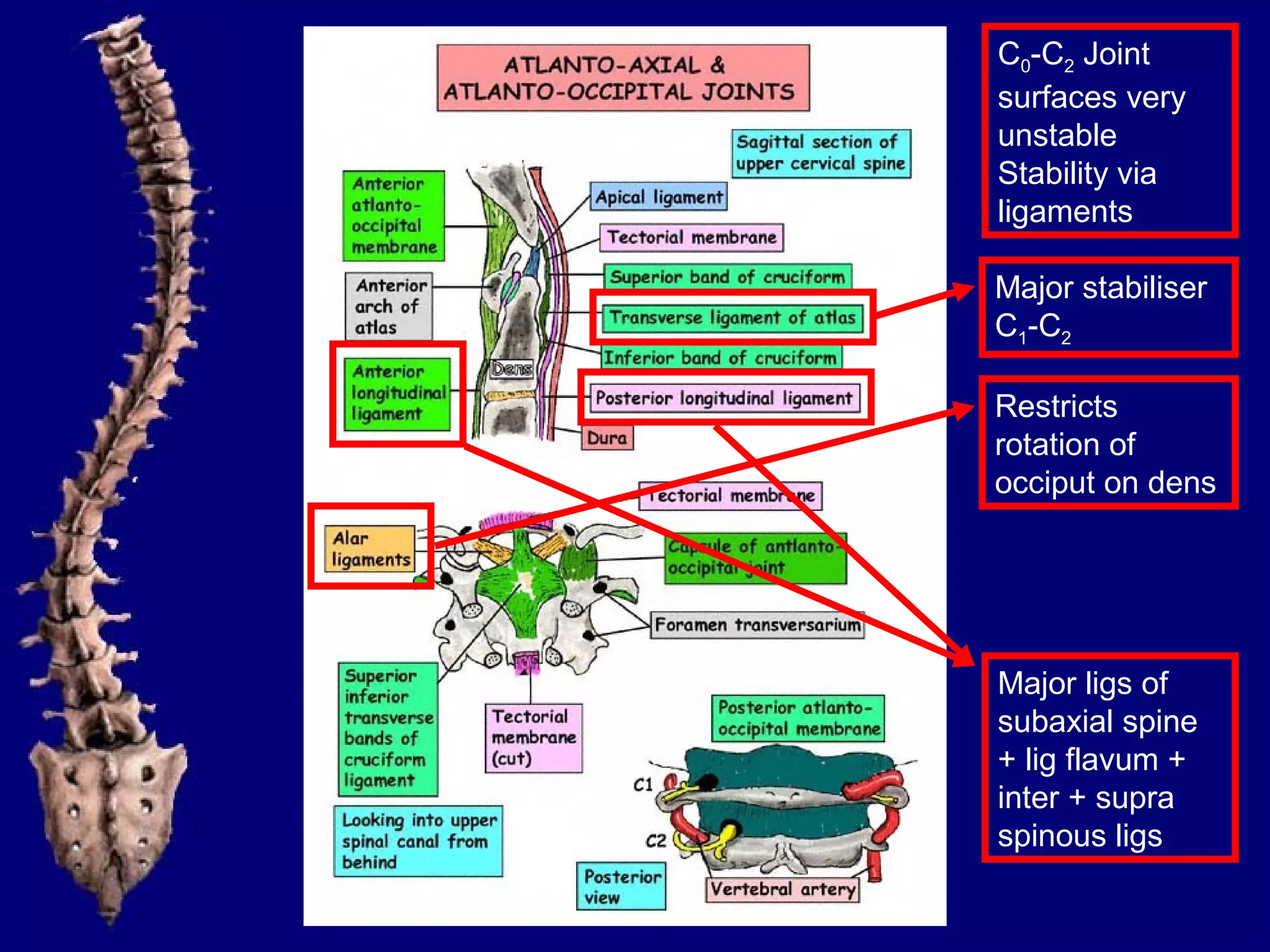
- Key concepts like clinical instability and relationships between structures.



















































































































![[3] The Back and ANS.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/3thebackandans-230325182407-aaf75a6c-thumbnail.jpg?width=640&height=640&fit=bounds)











































