This document discusses several pediatric gastrointestinal conditions:
- Testicular torsion presents with severe testicular or abdominal pain and requires surgical fixation following reduction to prevent recurrence.
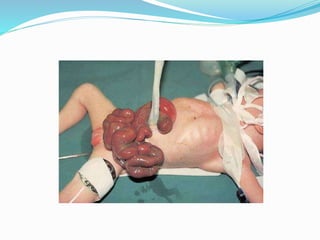
- Exomphalos involves intestinal loops protruding in a sac through an abdominal wall defect, with prognosis depending on associated anomalies.
- Gastroschisis has intestines protruding without a sac and fewer associated anomalies.
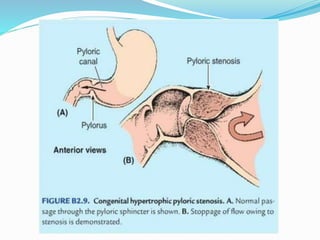
- Pyloric stenosis causes projectile vomiting in infants around 6 weeks and is treated surgically.